CARE Fertility & Women’s Health
May 2025
Disclaimer: Please note that this medical review is intended for informational purposes only and should not be considered as medical advice. It has been prepared with the assistance of artificial intelligence and has not undergone peer review by medical professionals. Consult with a qualified healthcare provider for personalized medical guidance and treatment. The information provided herein is not a substitute for professional medical advice.
Abstract
Conventional In Vitro Fertilization (IVF) and Intracytoplasmic Sperm Injection (ICSI) are mainstays of assisted reproductive technology (ART), each developed to address distinct aspects of infertility. Conventional IVF, which involves co-incubation of oocytes and sperm, was initially established for female infertility, particularly tubal factor disease. ICSI, a more invasive technique where a single sperm is injected directly into an oocyte, revolutionized the treatment of severe male factor infertility. While ICSI is indispensable for such cases, its application has expanded significantly to non-male factor infertility (NMFI), a practice that remains controversial due to a lack of consistent evidence demonstrating improved live birth rates (LBR). This review provides a comprehensive comparison of conventional IVF and ICSI, examining their historical development, laboratory procedures, clinical indications, and comparative efficacy regarding fertilization, embryo quality, implantation, clinical pregnancy, and live birth rates. It further delves into the safety profiles for both mother and offspring, including congenital, genetic, epigenetic, and neurodevelopmental considerations. Economic analyses highlight ICSI's increased cost, questioning its cost-effectiveness in NMFI. Ethical considerations surrounding patient autonomy, resource allocation, and the "ICSI paradox" – the potential transmission of genetic defects – are discussed in the context of professional guidelines from bodies like the American Society for Reproductive Medicine (ASRM) and the European Society of Human Reproduction and Embryology (ESHRE). The review underscores the necessity of evidence-based decision-making and individualized patient counseling to ensure the appropriate application of these powerful reproductive technologies.
1. Introduction
1.1. Background on Assisted Reproductive Technologies (ART)
Assisted Reproductive Technologies (ART) encompass a range of medical procedures designed to help individuals and couples overcome infertility, a condition affecting approximately 12–15% of couples of reproductive age.¹ These technologies involve the manipulation of gametes (sperm and oocytes) or embryos outside the human body to achieve pregnancy.² The evolution of ART represents a significant medical advancement, offering hope to many facing challenges with natural conception due to various pathological obstacles in both males and females, such as blocked fallopian tubes, ovulatory dysfunction, or sperm abnormalities.² This continuous drive to overcome biological limitations has led to the development and refinement of various techniques, but this progress sometimes outpaces the rigorous establishment of evidence for new applications or the expanded use of existing technologies, necessitating ongoing critical evaluation.
1.2. Emergence and Rationale for Conventional IVF and ICSI
Conventional In Vitro Fertilization (IVF) stands as a foundational ART. Its clinical emergence, marked by the birth of Louise Brown in 1978, was initially targeted at female infertility, predominantly tubal disease.³ The procedure involves retrieving oocytes and co-incubating them with a prepared sperm sample in a laboratory dish, allowing fertilization to occur in vitro.⁴ This method relies on the intrinsic ability of sperm to penetrate and fertilize the oocyte.
Intracytoplasmic Sperm Injection (ICSI) is a more specialized ART technique developed later, in the early 1990s.⁴ It involves the direct microinjection of a single, selected spermatozoon into the cytoplasm of a mature oocyte.³ ICSI was primarily developed to overcome severe male factor infertility, where sperm counts are extremely low, motility is poor, morphology is abnormal, or where sperm must be surgically retrieved, conditions under which conventional IVF is likely to fail or is not feasible.¹ By directly injecting the sperm, ICSI bypasses several natural physiological barriers to fertilization, including the cumulus oophorus, zona pellucida, and oolemma, as well as the natural sperm selection mechanisms that occur in vivo and to some extent in conventional IVF.¹ The distinct origins and primary rationales for IVF and ICSI are crucial for understanding the subsequent debates about their appropriate application; IVF aimed to bypass tubal blockage, while ICSI was designed to overcome sperm dysfunction at the very point of fertilization.
1.3. Objectives of the Review
This review aims to provide a comprehensive, evidence-based comparison of conventional IVF and ICSI. It will cover their historical development, detailed laboratory methodologies, established and debated clinical indications, and comparative efficacy in terms of fertilization, embryo development, implantation, clinical pregnancy, and live birth rates. Furthermore, the review will scrutinize the safety profiles of both techniques for the mother and offspring, including obstetric risks, and short-term and long-term health outcomes for children, encompassing congenital, genetic, epigenetic, and neurodevelopmental aspects. Economic considerations, such as cost-effectiveness and the financial impact of ICSI overuse, will be analyzed. Finally, ethical implications, including patient autonomy, resource allocation, and adherence to professional guidelines from organizations like ASRM and ESHRE, will be discussed. A central focus will be the increasing use and ongoing debate surrounding ICSI for non-male factor infertility.⁴ The overarching goal is not merely to describe these techniques but to critically evaluate and synthesize current information, thereby offering insights that can inform clinical decision-making, guide patient counseling, and identify areas requiring further research in the dynamic field of reproductive medicine.
2. Historical Development
2.1. Milestones in Conventional IVF
The journey towards successful human IVF was a long and incremental one, built upon centuries of curiosity about reproduction and decades of scientific research. Early concepts can be traced back to ancient familiarity with artificial insemination (AI).⁹ The scientific pursuit gained momentum in the late 19th and early 20th centuries with animal experiments. Walter Heape reported the first known embryo transplantation in rabbits in the 1890s, and Gregory Pincus successfully fertilized rabbit eggs in vitro and implanted the resulting embryo in 1934.²
The pivotal breakthrough for human IVF came through the collaborative efforts of physiologist Robert G. Edwards and gynecologist Patrick Steptoe. Their persistent research, spanning over a decade, culminated in the birth of Louise Joy Brown on July 25, 1978, in the United Kingdom.² This event marked the dawn of clinical IVF, initially developed to treat female infertility caused by blocked or damaged fallopian tubes.³ Following this landmark achievement, IVF technology rapidly evolved. Key subsequent developments included the introduction of controlled ovarian stimulation protocols to retrieve multiple oocytes, the use of pelvic ultrasonography for monitoring follicular growth and guiding oocyte retrieval, significant improvements in embryo culture media, and the establishment of embryo cryopreservation techniques, which allowed for the storage of surplus embryos and improved cumulative pregnancy rates.² This gradual, multi-step process, rooted in extensive research in reproductive physiology, endocrinology, and embryology, established IVF as a cornerstone of infertility treatment well before more targeted micromanipulation techniques emerged.
2.2. Development and Introduction of ICSI
The advent of ICSI was a direct response to the limitations of conventional IVF, particularly its low success rates in cases of severe male factor infertility. Prior to ICSI, various micromanipulation techniques were explored to assist sperm in fertilizing the oocyte, such as Partial Zona Dissection (PZD), which involved mechanically creating an opening in the zona pellucida, and Subzonal Insemination (SUZI), where sperm were placed directly into the perivitelline space.¹ However, these earlier methods had inconsistent success and often resulted in suboptimal fertilization rates or polyspermy, especially in severe male infertility.¹
The conceptual and technical groundwork for ICSI was laid by experiments in animal models. Hiramoto first performed microinjection of spermatozoa into sea urchin eggs in 1962, followed by Lin's successful microinjection in mouse oocytes in 1966. Uehara and Yanagimachi, in 1976, observed sperm nucleus decondensation after microinjecting human or hamster sperm into hamster oocytes, furthering the understanding of the process.¹ The first live offspring from sperm-injected oocytes were reported in rabbits in 1988.¹
The definitive breakthrough for human ICSI occurred in 1992 when Gianpiero Palermo and colleagues at the Vrije Universiteit Brussel reported the first successful human pregnancies and births using the technique.¹ ICSI rapidly revolutionized the treatment landscape for male infertility, offering a viable path to biological parenthood for men with conditions previously considered untreatable, such as severe oligozoospermia (very low sperm count), asthenozoospermia (poor sperm motility), teratozoospermia (abnormal sperm morphology), and azoospermia (absence of sperm in the ejaculate), where sperm could be surgically retrieved from the epididymis (MESA/PESA) or testes (TESE).³ ICSI's targeted approach, directly addressing the sperm's inability to fertilize, explains its swift and widespread adoption for these specific indications. The inherently invasive nature of the technique, bypassing natural fertilization barriers, is central to both its success in severe male infertility and the subsequent concerns regarding its broader application and safety.
Table 1: Key Milestones in the Development of Conventional IVF and ICSI
Year(s) | Milestone | Key Figure(s)/Group | Technique | Significance | Reference(s) |
1890s | First embryo transplantation in rabbits | Walter Heape | IVF (animal) | Demonstrated feasibility of embryo transfer. | 2 |
1934 | In vitro fertilization and embryo implantation in rabbits | Gregory Pincus | IVF (animal) | Early demonstration of IVF and embryo development. | 2 |
1959 | First undeniable evidence of in vitro fertilization leading to live birth in rabbits | Min Chueh Chang | IVF (animal) | Confirmed feasibility of IVF leading to live birth. | 2 |
1962 | Microinjection of spermatozoa into sea urchin eggs | Hiramoto | ICSI (animal) | Early pioneering work in sperm microinjection. | 1 |
1973 | First reported human IVF pregnancy (early embryo death) | Carl Wood & John Leeton | IVF (human) | Early attempt at human IVF. | 2 |
1978 | Birth of Louise Brown, first human IVF baby | R. Edwards & P. Steptoe | IVF (human) | Landmark achievement; established clinical IVF for human infertility (tubal disease). | 2 |
1984 | Birth of Zoe Leyland, first baby from a frozen-thawed embryo | A. Trounson & C. Wood | IVF (human) | Demonstrated viability of cryopreserved embryos, expanding IVF flexibility. | 2 |
1988 | First live offspring in rabbits after ICSI | - | ICSI (animal) | Demonstrated ICSI could lead to live birth in mammals. | 1 |
Early 1990s | Development of ICSI for human application | G. Palermo & colleagues | ICSI (human) | Overcame limitations of conventional IVF for severe male infertility. | 1 |
1992 | First reported human births using ICSI | G. Palermo & colleagues | ICSI (human) | Revolutionized treatment for severe male factor infertility, offering new hope for biological parenthood. | 1 |
3. Methodological Overview: Conventional IVF vs. ICSI
3.1. Ovarian Stimulation, Oocyte Retrieval, and Embryo Culture (Common Aspects)
The initial clinical and laboratory phases are largely identical for both conventional IVF and ICSI cycles. The process typically begins with controlled ovarian stimulation (COS). Women receive hormonal medications, such as gonadotropin-releasing hormone (GnRH) agonists or antagonists to prevent premature ovulation, and gonadotropins (follicle-stimulating hormone (FSH) and/or luteinizing hormone (LH)) to stimulate the ovaries to produce multiple follicles.¹⁰ The response to stimulation is closely monitored through transvaginal ultrasound scans to measure follicular growth and blood tests to assess estradiol levels.¹⁰
Once follicles reach an optimal size, a final maturation trigger (e.g., human chorionic gonadotropin (hCG) or a GnRH agonist) is administered, and oocyte retrieval is scheduled approximately 34–36 hours later.¹⁰ Oocyte retrieval is a minimally invasive procedure, usually performed under sedation, where oocytes are aspirated from the ovarian follicles using an ultrasound-guided needle.¹¹
Retrieved oocytes are then transferred to the embryology laboratory. Here, they are assessed for maturity, and subsequent steps diverge based on whether conventional IVF or ICSI is planned.¹² Following fertilization (by either method), the resulting embryos are cultured in a strictly controlled laboratory environment that mimics the conditions of the human body. Embryos are monitored for development and graded based on morphological criteria over several days (typically 3 to 7 days).¹² The highest quality embryo(s) are then selected for transfer into the woman's uterus, while surplus viable embryos may be cryopreserved for future use.¹¹ The commonality of these initial and concluding steps underscores that the primary distinction, and thus the focus of comparison and debate, lies specifically in the method employed to achieve fertilization of the oocytes.
3.2. Laboratory Procedures for Conventional IVF
3.2.1. Sperm Preparation Techniques
For conventional IVF, the collected semen sample must undergo preparation to isolate the healthiest, most motile sperm and remove seminal plasma, prostaglandins, non-motile sperm, cellular debris, and bacteria, which could be detrimental to fertilization or embryo development.¹² This process aims to capacitate the sperm, a physiological change sperm normally undergo in the female reproductive tract to become capable of fertilizing an egg. Common sperm preparation techniques include:
Swim-up: This technique relies on the active motility of sperm. The liquefied semen sample (or a washed pellet) is gently overlaid with a layer of culture medium. Motile sperm actively swim out of the seminal plasma or pellet into the clean medium. After an incubation period, the supernatant layer containing the motile sperm is collected.¹³ This method tends to select for sperm with good progressive motility.
Density Gradient Centrifugation (DGC): This method separates sperm based on their density. The semen sample is layered on top of one or more layers of colloidal silica solutions of different densities (e.g., a two-layer gradient of 40% and 80%, or 45% and 90%).¹⁴ During centrifugation, motile sperm with normal morphology, being denser, pass through the gradient layers and form a pellet at the bottom of the tube, while seminal plasma, debris, leukocytes, and abnormal or immotile sperm are retained in the upper layers.¹³ The resulting pellet is then washed and resuspended in culture medium. DGC is often preferred for samples with higher viscosity or debris.
The overarching goal of these preparation techniques is to yield a concentrated fraction of functionally competent spermatozoa, mimicking a natural selection process to some degree, for insemination of the oocytes.¹³ This contrasts with the ICSI approach, where a single sperm is selected by an embryologist.
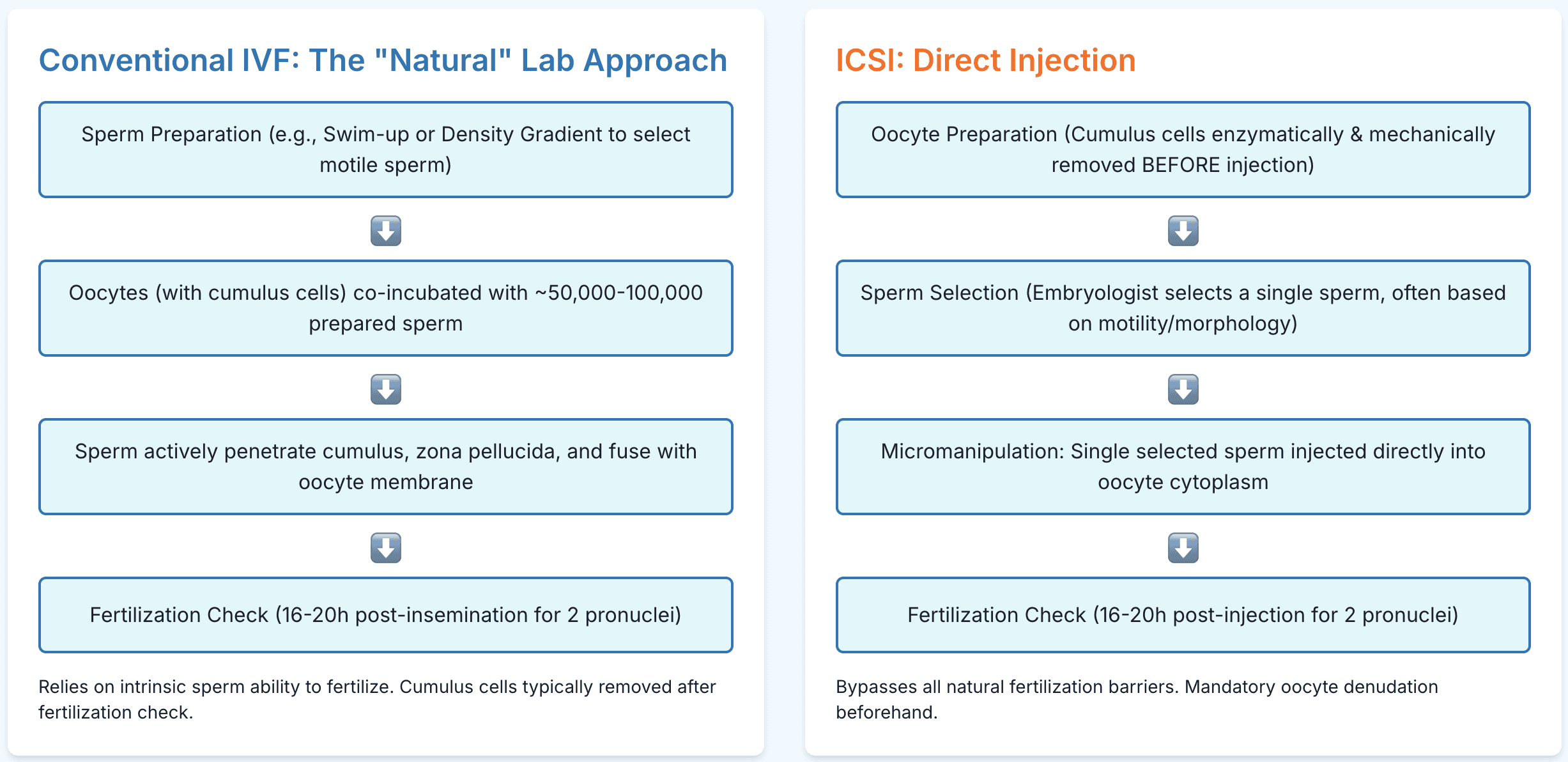
3.2.2. Oocyte Insemination and Fertilization Assessment
Following oocyte retrieval and sperm preparation, the mature oocytes (typically still surrounded by their cumulus cells) are placed into a culture dish containing specialized medium. A specific concentration of the prepared, motile sperm (usually around 50,000 to 100,000 sperm per oocyte) is added to the dish.⁴ The dish is then incubated under controlled conditions, allowing fertilization to occur "naturally" in the laboratory setting, where sperm must actively penetrate the cumulus complex, bind to and penetrate the zona pellucida, and fuse with the oolemma.⁴
Fertilization is assessed approximately 16–20 hours after insemination.¹⁷ At this point, the oocytes are examined under a microscope for the presence of two distinct pronuclei (2PN) – one derived from the oocyte and one from the sperm – and the extrusion of the second polar body. The presence of 2PN is the hallmark of normal fertilization.¹⁷ Oocytes showing no pronuclei are considered unfertilized, while those with one pronucleus (1PN) or three or more pronuclei (3PN, indicative of polyspermy) are considered abnormally fertilized and are typically not cultured further or are discarded.¹⁷ For conventional IVF, the cumulus cells are usually removed (denuded) after this incubation period, on the day of fertilization check, to allow clear visualization of the pronuclei.¹⁷ The sperm themselves will have contributed to loosening or removing much of the cumulus complex during the co-incubation period.¹⁷ This reliance on the inherent functional capacity of the sperm to achieve fertilization is a fundamental characteristic of conventional IVF, which ICSI entirely bypasses.
3.3. Laboratory Procedures for ICSI
3.3.1. Oocyte Preparation (Denudation)
Unlike conventional IVF, oocytes destined for ICSI must be completely denuded of their surrounding cumulus and corona radiata cells before the injection procedure.¹⁷ This denudation is essential for several reasons: it allows for the assessment of oocyte maturity (presence of the first polar body, indicating metaphase II stage), enables proper visualization of the oocyte cytoplasm for injection, and provides access for the micromanipulation pipettes.
The denudation process is typically a two-step procedure:
Enzymatic Treatment: Oocytes are briefly exposed to a dilute solution of hyaluronidase enzyme (e.g., 80 IU/mL) for a critical period, often around 30 seconds to 1 minute.¹⁷ Hyaluronidase breaks down the hyaluronic acid matrix that holds the cumulus cells together. Precise timing is crucial: insufficient exposure will result in incomplete cumulus removal, making ICSI impossible as the injection needle cannot pass through adherent cells; excessive exposure can be detrimental to the oocyte's viability.¹⁷
Mechanical Stripping: Following enzymatic treatment, the oocytes are mechanically stripped of remaining cumulus and corona cells. This is achieved by gently pipetting the oocytes through a series of glass pipettes with progressively smaller inner diameters (e.g., starting from around 175µm down to 135µm).¹⁷ The shear forces generated help to dislodge the remaining cells, leaving the oocyte "naked" and ready for injection.
This mandatory and meticulous denudation process for ICSI represents a more intensive and potentially stressful manipulation of the oocyte compared to conventional IVF, where sperm largely perform this role naturally. This increased handling is a point of consideration for potential oocyte stress or damage.
3.3.2. Sperm Selection
After sperm preparation (often using similar methods as for conventional IVF, such as DGC, especially if starting from a raw semen sample¹⁵), a single spermatozoon must be selected for injection into each mature oocyte. In standard ICSI, this selection is typically performed by an embryologist under an inverted microscope at magnifications of 200x to 400x.¹¹ The embryologist assesses sperm based primarily on motility and gross morphology.
To facilitate selection and handling, the viscosity of the medium containing the sperm is often increased using polyvinylpyrrolidone (PVP).¹⁵ This slows down the sperm, making it easier to aspirate an individual motile sperm into the injection pipette. Before aspiration, the selected sperm is usually immobilized by gently striking its tail with the tip of the injection pipette or by aspirating it vigorously against the bottom of the dish; this is thought to aid in the release of sperm-borne oocyte-activating factors.⁴
Recognizing the limitations and subjectivity of conventional sperm selection, which may contribute to the "ICSI paradox" (the potential transmission of genetically defective sperm by bypassing natural selection mechanisms³), advanced sperm selection techniques have been developed. These include:
Intracytoplasmic Morphologically Selected Sperm Injection (IMSI): This technique employs high-magnification microscopy (typically >6000x) using differential interference contrast (DIC) optics to allow for detailed assessment of sperm morphology, particularly the presence and nature of vacuoles in the sperm head, which may be associated with DNA damage or aneuploidy.¹⁵ Specialized equipment, including inverted microscopes with DIC capabilities and high-power objectives, is required.¹⁵
Other Emerging Technologies: Research is ongoing into other methods to improve sperm selection, such as microfluidic sperm sorting (which aims to mimic aspects of natural sperm selection in the female reproductive tract), quantitative analysis of sperm DNA fragmentation, sperm proteomics, and non-invasive imaging techniques like quantitative phase microscopy (QPM) for objective sperm assessment.³
The reliance on visual morphological assessment at standard magnifications in routine ICSI has been termed part of "andrological ignorance," where deeper functional or genetic sperm defects may be overlooked.³ Advanced methods aim to refine this crucial selection step, though their widespread adoption is limited by factors such as cost, time, and the need for further validation of clinical benefit.
3.3.3. Micromanipulation and Injection Technique
The ICSI procedure itself is performed using a specialized setup consisting of an inverted microscope equipped with micromanipulators. These manipulators control a holding pipette and an injection pipette.⁴
Oocyte Immobilization: A mature, denuded oocyte is secured by gentle suction using the holding pipette. The oocyte is typically oriented with its polar body at the 6 or 12 o’clock position to avoid damaging the meiotic spindle, which is usually located nearby.⁴
Sperm Aspiration and Injection: The selected and immobilized sperm is aspirated, usually tail-first, into the fine, sharp-tipped glass injection pipette.⁴ The embryologist then carefully guides the injection pipette to pierce the zona pellucida and then the oolemma (oocyte membrane) at the 3 o’clock position. The sperm is then gently expelled into the ooplasm (cytoplasm of the oocyte).¹ A small amount of ooplasm is typically aspirated into the injection pipette before sperm expulsion to ensure that the oolemma has been breached and to facilitate sperm release; this also helps to initiate oocyte activation.⁴ The entire procedure for a single oocyte usually takes between 2 to 4 minutes.⁴
Oocyte Activation: The mechanical act of injection and the introduction of sperm cytosolic factors, along with the influx of extracellular calcium from the injection medium, typically triggers the cascade of events leading to oocyte activation.⁶ This activation includes calcium oscillations within the ooplasm, resumption of meiosis II, and ultimately, pronuclear formation.
The ICSI injection is a highly skilled and invasive procedure that physically bypasses all of the oocyte’s natural protective barriers and selection mechanisms. While profoundly effective in overcoming severe fertilization barriers, this direct intervention carries inherent risks of physical damage to the oocyte (though low in experienced hands, estimated around 5–10%¹⁶) and eliminates the complex molecular dialogue that normally occurs between sperm and oocyte during natural fertilization.
Table 2: Comparison of Laboratory Procedures: Conventional IVF vs. ICSI
Feature | Conventional IVF | Intracytoplasmic Sperm Injection (ICSI) | Reference(s) |
Oocyte State at Insemination | Cumulus-oocyte complex (cumulus cells usually present) | Denuded oocyte (cumulus and corona cells removed) | 17 |
Sperm Preparation Goal | Obtain a population of motile, capacitated sperm for co-incubation | Select a single, morphologically normal, motile (then immobilized) sperm for injection | 11 |
Sperm Number Used | Approx. 50,000-100,000 motile sperm per oocyte | One sperm per oocyte | 4 |
Method of Fertilization | Co-incubation of oocytes and sperm; sperm penetrates oocyte "naturally" in vitro | Microinjection of a single sperm directly into the oocyte cytoplasm | 1 |
Oocyte Denudation | Performed after fertilization check (Day 1) to visualize pronuclei | Performed before injection (Day 0) to assess maturity and allow micromanipulation | 17 |
Natural Barriers Bypassed | Sperm must penetrate cumulus, zona pellucida, and fuse with oolemma | All natural barriers (cumulus, zona, oolemma) are mechanically bypassed by the injection pipette | 1 |
Key Equipment/Reagents | Standard culture dishes, incubators, sperm preparation media | As for IVF, plus: micromanipulator system, holding/injection pipettes, hyaluronidase, PVP (often) | 4 |
Invasiveness | Less invasive for the oocyte | More invasive; direct physical penetration of the oocyte | 4 |
Sperm Selection | Relies on sperm's intrinsic ability and some in vitro selection during prep | Embryologist selects a single sperm based on motility/morphology (standard) or advanced criteria (IMSI) | 3 |
4. Clinical Indications
4.1. Indications for Conventional IVF
Conventional IVF has historically been, and continues to be, a cornerstone treatment for a wide array of infertility causes, primarily those where the spermatozoa are considered capable of fertilizing an oocyte if provided access in a laboratory setting. Key indications include⁵:
Tubal factor infertility: This was the original indication for IVF, where damage or blockage of the fallopian tubes prevents the natural meeting of sperm and egg.³
Endometriosis: Women with endometriosis, particularly moderate to severe stages, may benefit from IVF if other treatments have failed or are not appropriate.⁵
Ovulatory disorders: While ovulation induction is often a first-line treatment, IVF may be used for refractory anovulation or when combined with other factors.⁵
Unexplained infertility: When a standard infertility evaluation fails to identify a specific cause, IVF is often offered after less invasive treatments have been unsuccessful.⁵
Moderate male factor infertility: Cases where sperm parameters are suboptimal but not severe enough to preclude fertilization with conventional insemination techniques in vitro.⁵
Diminished ovarian reserve: While success rates may be lower, IVF can be an option for women with a reduced number of oocytes.²¹
Uterine or peritoneal factors: Certain uterine anomalies or peritoneal adhesions may necessitate IVF.
Cervical factor infertility: Though less common with the advent of IUI and IVF.
Failed IUI cycles: Couples who have not conceived after several cycles of intrauterine insemination may proceed to IVF.
The American Society for Reproductive Medicine (ASRM) also lists conditions such as irregular menstrual cycles, known or suspected uterine/tubal/peritoneal disease, certain cases of male subfertility, sexual dysfunction, and genetic or acquired conditions predisposing to diminished ovarian reserve as situations where an infertility evaluation, potentially leading to IVF, should be considered.²¹ Conventional IVF remains the foundational ART for these broad categories, assuming that sperm function is adequate for in vitro fertilization.
4.2. Primary Indications for ICSI: Severe Male Factor Infertility
There is unanimous consensus within the reproductive medicine community that Intracytoplasmic Sperm Injection (ICSI) is the indicated and revolutionary treatment for severe male factor infertility (SMFI).⁴ This is the primary context for which ICSI was developed and where its benefits are most clearly established. SMFI encompasses a range of significant abnormalities in sperm parameters, often defined according to World Health Organization (WHO) criteria²³, which render conventional IVF unlikely to succeed. These include:
Severe Oligozoospermia: Very low sperm concentration, for example, less than 5 million sperm per milliliter of ejaculate²⁵, or a post-wash total progressively motile sperm count of less than 1 million.²⁶
Severe Asthenozoospermia: Markedly reduced sperm motility, where a very low percentage of sperm are capable of progressive movement necessary to reach and penetrate the oocyte.⁵
Severe Teratozoospermia: A very high percentage of abnormally shaped sperm, often defined as less than 4% normal forms according to strict Kruger criteria.²⁶
Azoospermia: The complete absence of sperm in the ejaculate. This can be:
Obstructive Azoospermia (OA): Caused by a blockage in the reproductive tract (e.g., congenital bilateral absence of the vas deferens (CBAVD) or previous vasectomy), where sperm production is normal but sperm cannot be ejaculated. In these cases, sperm can be surgically retrieved from the epididymis (Microsurgical Epididymal Sperm Aspiration - MESA; Percutaneous Epididymal Sperm Aspiration - PESA) or testes (Testicular Sperm Extraction - TESE).³
Non-Obstructive Azoospermia (NOA): Caused by testicular failure, where sperm production is severely impaired or absent. Sperm may still be found in focal areas of the testes and retrieved via TESE (often micro-TESE) in a proportion of these men.³
Cryptozoospermia: Extremely few sperm found in the ejaculate, often only after centrifugation of the pellet.²⁹
Presence of High Titers of Antisperm Antibodies (ASAs): When ASAs are present in significant levels, they can interfere with sperm motility, capacitation, or sperm-oocyte binding, making conventional IVF difficult.²⁶
Previous Total Fertilization Failure (TFF) or Very Low Fertilization with Conventional IVF: This is a strong indication, even if baseline semen parameters are not severely abnormal, as it suggests an underlying sperm-oocyte interaction defect that ICSI can bypass.⁴
In all these scenarios, ICSI’s ability to bypass natural fertilization barriers by directly injecting a single sperm into the oocyte makes it an effective intervention, offering a chance of biological parenthood that was previously unattainable for many men with SMFI.³
4.3. Expanding Use of ICSI: Non-Male Factor Infertility (NMFI)
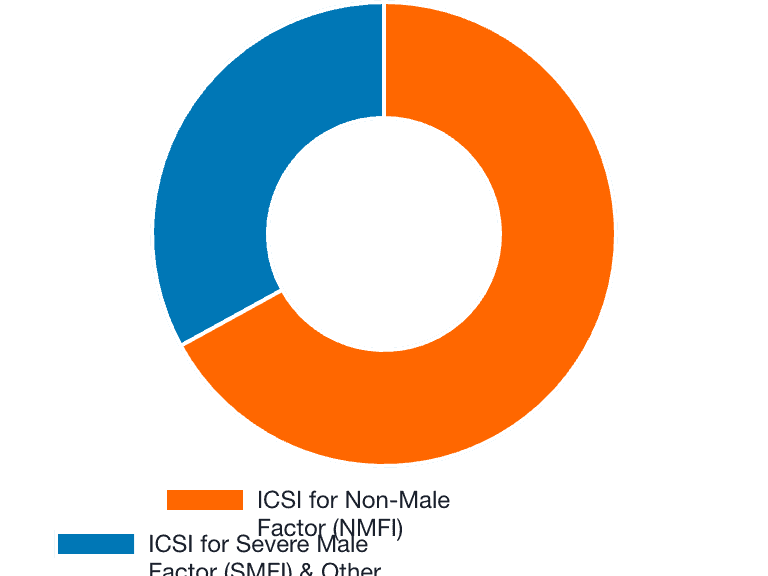
Despite its development for SMFI, the use of ICSI has dramatically expanded to include a wide range of non-male factor infertility (NMFI) indications. Data from the US showed an increase in ICSI for NMFI from 15.4% of such cycles in 1996 to 66.9% in 2012⁷, and in some settings, ICSI accounts for up to 80% of all ART cycles performed.³ This trend of "ICSI-for-all" or "routine ICSI" is observed globally.³²
This expansion is highly controversial and often deviates from evidence-based guidelines. Major professional bodies like ASRM and ESHRE advise caution or explicitly recommend against the routine use of ICSI in NMFI in the absence of specific supporting indications.⁴ The National Institute for Health and Care Excellence (NICE) guidelines in the UK also stipulate that ICSI should primarily be used for severe deficits in sperm quality or following a previous IVF cycle with failed or very poor fertilization.³³
The rationale behind this widespread "indication creep" is multifactorial. A primary driver is the desire to avoid total fertilization failure (TFF), which can occur in a small percentage of conventional IVF cycles even with normal sperm parameters.⁷ Other contributing factors may include perceived laboratory efficiency, clinician or embryologist preference, patient request, and, in some healthcare systems, financial incentives or disincentives related to reimbursement policies.⁷ This divergence between widespread clinical practice and evidence-based recommendations forms a central point of debate in modern ART.
4.3.1. Unexplained Infertility
Proposed Rationale: In cases of unexplained infertility, where no specific cause for infertility is identified after standard investigations, it is sometimes hypothesized that ICSI might bypass potential, yet undiagnosed, barriers to fertilization at the gamete level.³¹
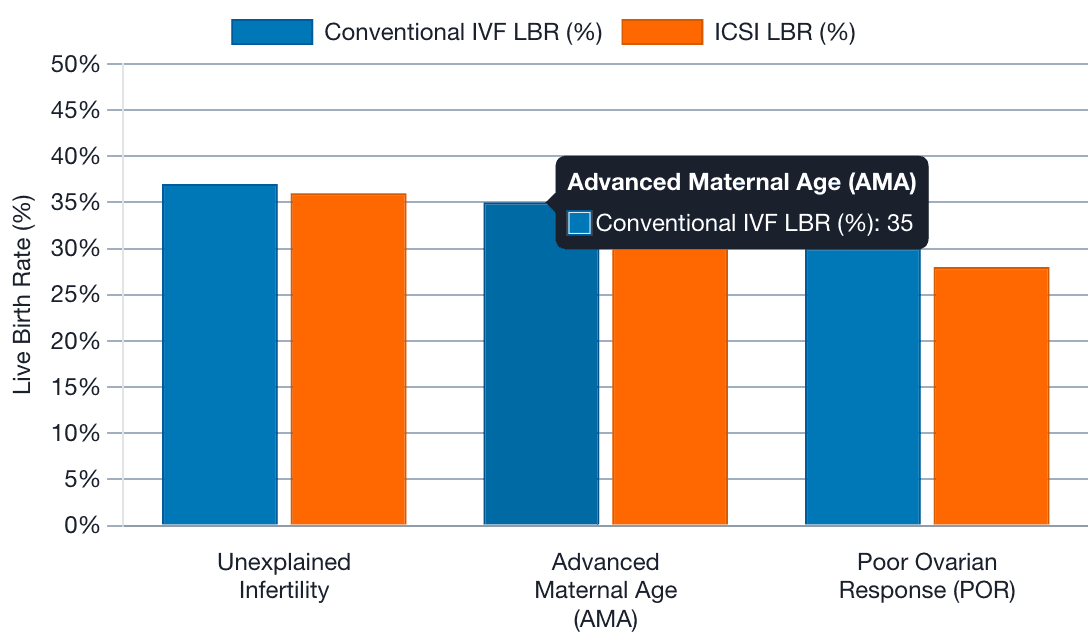
Evidence: Some studies, particularly those using a sibling oocyte design (where oocytes from the same patient are randomly allocated to either conventional IVF or ICSI), have reported increased fertilization rates and a decreased risk of TFF with ICSI in this population.³¹ However, a critical review of these studies suggests that the benefit in reducing TFF is more pronounced in sibling oocyte studies, which may be prone to certain biases, than in patient-randomized trials.⁸ More importantly, numerous randomized controlled trials (RCTs) and meta-analyses have generally failed to demonstrate an improvement in the ultimate outcome of live birth rates (LBR) when ICSI is used for unexplained infertility compared to conventional IVF.⁸ The ASRM committee opinion states that while ICSI for unexplained infertility has been associated with increased fertilization rates in some studies, the evidence for benefit is limited, and it has not been shown to improve LBR.³¹ The "unknown" nature of unexplained infertility makes it an attractive target for more interventionist approaches like ICSI. However, the consistent lack of LBR improvement suggests that if fertilization itself is not the primary rate-limiting step for these couples, then ICSI offers no tangible advantage and may introduce unnecessary procedural complexity, risks, and costs.
4.3.2. Advanced Maternal Age (AMA)
Proposed Rationale: It has been theorized that oocytes from women of advanced maternal age (typically defined as ≥ 35 or ≥ 38 years) may exhibit age-related structural changes, such as hardening of the zona pellucida or cytoplasmic defects, which could impair sperm penetration and fertilization with conventional IVF techniques.⁷ ICSI is therefore proposed to overcome these potential barriers.
Evidence: Despite these theoretical concerns, oocyte fertilization rates with conventional IVF in AMA women are often comparable to those observed in younger women.³¹ Multiple studies, including retrospective analyses and systematic reviews, have shown no significant improvement in LBR with the routine use of ICSI for AMA when male factor infertility is absent.⁷ The ASRM committee opinion explicitly states that ICSI for AMA does not improve LBR.³¹ The primary challenge in AMA is often diminished oocyte quality, particularly an increased incidence of aneuploidy (chromosomal abnormalities), which ICSI cannot correct and which is a major determinant of implantation failure and early pregnancy loss. Focusing on the method of fertilization via ICSI in AMA cases may therefore be a misdirection from the core issue of oocyte competence.
4.3.3. Poor Ovarian Response (POR) / Low Oocyte Yield
Proposed Rationale: In women classified as poor ovarian responders or those who yield a low number of oocytes after stimulation, ICSI is sometimes employed with the aim of maximizing the fertilization rate and thus the number of embryos available for transfer or cryopreservation from the limited cohort of retrieved oocytes.⁷
Evidence: The evidence supporting this practice is weak and often contradictory. While some studies might show an increased fertilization rate per injected oocyte with ICSI, this does not consistently translate into improved LBR. Several controlled trials and large retrospective analyses have found similar or even lower LBR with ICSI compared to conventional IVF in POR or low oocyte yield patients without male factor infertility.⁷ The ASRM committee opinion concludes that ICSI for low oocyte yield does not improve LBR.³¹ One notable large study found that while ICSI significantly increased the 2PN fertilization rate irrespective of the number of oocytes retrieved (1–3, 4–6, or 7–9), conventional IVF cycles demonstrated higher implantation rates, clinical pregnancy rates, and live birth rates, particularly when three or fewer oocytes were retrieved.⁴⁵ In POR, oocyte quality is frequently a concern alongside quantity. The more invasive nature of ICSI might not be beneficial, and could potentially be detrimental, to the few, possibly already compromised, oocytes available. Alternatively, oocytes from POR patients that are robust enough to fertilize via conventional IVF may represent a cohort with inherently better developmental potential.
4.3.4. Previous Fertilization Failure (PFF) or Low Fertilization with Conventional IVF
Proposed Rationale: This is considered one of the strongest NMFI indications for ICSI.²⁶ If a couple has experienced total fertilization failure or a very low fertilization rate (<20–30%) in a previous conventional IVF cycle despite apparently normal semen parameters, it suggests an underlying, possibly unidentified, sperm-oocyte interaction defect or a functional sperm deficiency that prevents successful fertilization through natural mechanisms in vitro. ICSI is used in subsequent cycles to directly bypass these potential barriers.
Evidence: ICSI has been shown to significantly increase fertilization rates in subsequent ART cycles for couples with a history of PFF or unexpectedly low fertilization with conventional IVF.³¹ Both ASRM and NICE guidelines support the use of ICSI in this specific scenario.³¹ This indication is logical because there is a demonstrated problem with fertilization using conventional IVF for that particular couple; ICSI directly addresses this established block by ensuring sperm entry into the oocyte. This contrasts with other NMFI scenarios where no such fertilization impediment has been previously proven.
4.3.5. Use with Preimplantation Genetic Testing (PGT)
Proposed Rationale: ICSI has been traditionally recommended when PGT is planned, particularly for PGT for monogenic diseases (PGT-M) which often relies on polymerase chain reaction (PCR) based amplification of DNA from biopsied embryonic cells.³¹ The primary concern is to prevent contamination of the embryo biopsy sample with extraneous, non-fertilizing sperm that may be loosely attached to the zona pellucida in conventional IVF. Such contamination could lead to misdiagnosis.³¹
Evidence: The ASRM committee opinion suggests that ICSI for PGT in the absence of male factor infertility should be limited to cases where contamination of extraneous sperm could genuinely affect the accuracy of the test results, such as with some PCR-based assays.³¹ With the increasing use of newer molecular techniques for PGT, such as Next-Generation Sequencing (NGS) for PGT for aneuploidy (PGT-A), the risk and impact of minor sperm contamination may be less critical.³¹ A recent study evaluating PGT-A on frozen-thawed embryos found no difference in blastocyst euploidy rates, clinical outcomes, or accuracy of PGT-A results between embryos derived from conventional IVF versus ICSI, and notably, no parental contamination was detected in the conventional IVF group.⁴⁷ This suggests that for certain PGT applications, especially PGT-A on thawed embryos, the routine use of ICSI solely to prevent contamination may not be necessary if laboratory protocols for embryo washing are robust. The decision often becomes a laboratory-specific protocol consideration rather than a direct therapeutic benefit for the embryo's developmental potential itself.
4.3.6. Use with Cryopreserved or In Vitro Matured (IVM) Oocytes
Cryopreserved Oocytes: ICSI is generally the preferred method of fertilization for previously cryopreserved (vitrified) oocytes.¹⁶ The rationale is that the oocyte cryopreservation process, which typically involves denuding the oocytes of cumulus cells prior to freezing, and the freeze-thaw process itself, might alter the zona pellucida, potentially hardening it or otherwise impairing its receptivity to sperm in conventional IVF.³¹ The ASRM committee opinion states that ICSI on cryopreserved oocytes is the preferred method, although it acknowledges that limited comparative data currently exist to definitively support this procedure over conventional IVF in all cases.³¹ A retrospective analysis of thawed vitrified embryos found no difference in live birth rates between embryos derived from IVF versus ICSI⁴⁸, suggesting that the post-thaw developmental competence of embryos might be similar regardless of the initial fertilization method if fertilization is achieved.
In Vitro Matured (IVM) Oocytes: ICSI has also been advocated for oocytes matured in vitro from an immature (germinal vesicle or metaphase I) stage.¹⁶ Similar to cryopreserved oocytes, the concern is that the IVM process might lead to changes in the zona pellucida that could hinder fertilization by conventional IVF. The evidence here is mixed; some studies suggest ICSI improves fertilization rates of IVM oocytes. However, other data indicate that conventional IVF might yield better implantation and clinical pregnancy rates with IVM oocytes, although comprehensive LBR data are often lacking.³¹
For both cryopreserved and IVM oocytes, the rationale for ICSI is largely based on presumed oocyte alterations that could compromise conventional IVF. While ICSI might appear to be a pragmatic choice due to these manipulations, more robust research, particularly focusing on LBR, is needed to confirm clear and consistent benefits over conventional IVF if sperm parameters are normal.
Table 3: Summary of Clinical Indications for Conventional IVF and ICSI (Including ASRM/ESHRE/NICE Recommendations for Non-Male Factor ICSI)
Indication Category | Specific Indication | Conventional IVF Recommended | ICSI Recommended | Guideline Consensus (ASRM/ESHRE/NICE for NMFI ICSI) | Reference(s) |
Female Factor | Tubal disease | Yes | No (unless MFI also present) | N/A (IVF is primary) | 3 |
Endometriosis | Yes | No (unless MFI also present or PFF with IVF) | N/A (IVF is primary) | 5 | |
Ovulatory dysfunction (refractory) | Yes | No (unless MFI also present) | N/A (IVF is primary) | 5 | |
Male Factor | Moderate male factor | Yes | Consider if IVF fails or borderline parameters | N/A | 5 |
Severe Male Factor Infertility (SMFI) (Oligo-, Astheno-, Terato-zoospermia, Azoospermia, Cryptozoospermia, ASAs) | No | Yes (Primary Indication) | Strong consensus: ICSI is treatment of choice. | 3 | |
Non-Male Factor (NMFI) | Unexplained infertility | Yes (often first ART line) | No (Routine use not recommended) | ASRM: No LBR improvement, limited evidence. ESHRE/NICE: Not for routine use. | 8 |
Advanced Maternal Age (AMA) | Yes | No (Routine use not recommended) | ASRM: No LBR improvement. ESHRE/NICE: Not for routine use based on age alone. | 7 | |
Poor Ovarian Response (POR) / Low Oocyte Yield | Yes | No (Routine use not recommended) | ASRM: No LBR improvement. ESHRE/NICE: Not for routine use based on POR alone. | 7 | |
Previous Fertilization Failure (PFF) with cIVF | No (for subsequent cycle) | Yes | Strong consensus: ICSI is indicated after PFF with cIVF. | 4 | |
Preimplantation Genetic Testing (PGT) | Yes (can be used) | Often used, especially for PGT-M (PCR based) | ASRM: Limit to cases where contamination affects results. ESHRE/NICE: Consider if needed to prevent contamination. Necessity declining with newer PGT techniques. | 22 | |
Cryopreserved Oocytes | Less common | Often Preferred | ASRM: Preferred method, limited data. ESHRE/NICE: Considered standard practice by many labs due to zona changes. | 16 | |
In Vitro Matured (IVM) Oocytes | Possible | Often used | ASRM: Improves FR, but CPR/IR may be higher with cIVF; LBR data lacking. ESHRE/NICE: Use based on lab protocol/evidence. | 16 |
5. Comparative Efficacy and Clinical Outcomes
The comparative efficacy of conventional IVF and ICSI is a subject of extensive research and debate, particularly when ICSI is applied to non-male factor infertility (NMFI). Outcomes such as fertilization rates, embryo quality, implantation rates, clinical pregnancy rates, and, most importantly, live birth rates (LBR) are key metrics in this comparison.
5.1. Fertilization Rates (FR)
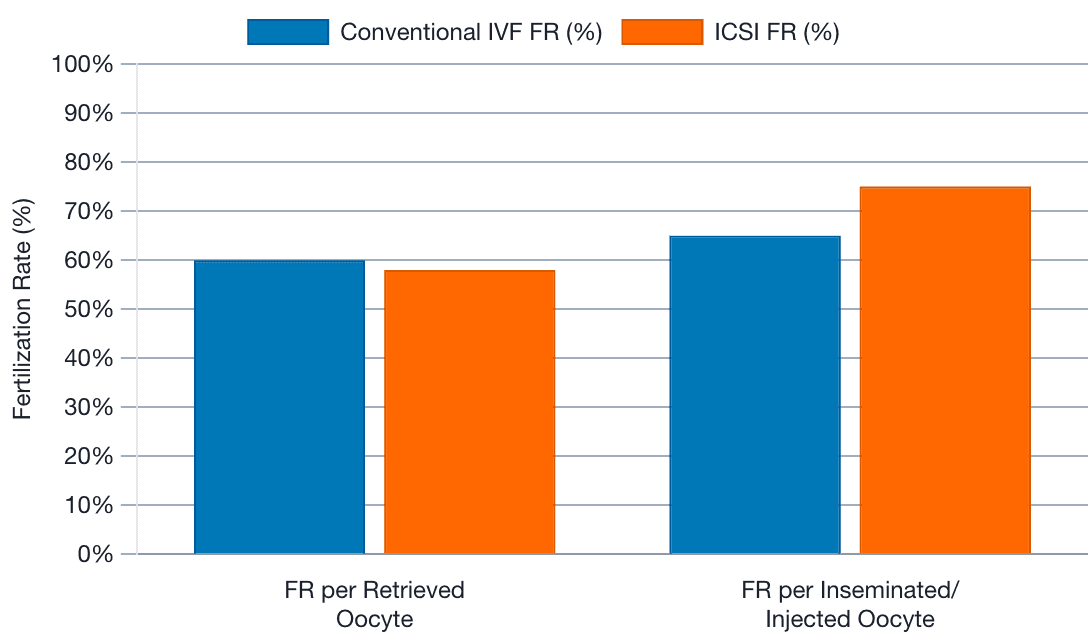
ICSI is known to achieve high fertilization rates, typically between 65% and 80% with ejaculated spermatozoa, provided the sperm is viable, largely independent of its functional capacity in natural fertilization.¹ This is a direct consequence of bypassing natural barriers. In contrast, conventional IVF fertilization rates can be more variable and are susceptible to total fertilization failure (TFF), which has been reported to occur in 5–20% of cycles in some studies, even with apparently normal sperm.⁵⁰
In the context of NMFI, the data on fertilization rates are mixed. Some studies, particularly those employing a sibling oocyte design, suggest that ICSI may increase FR and reduce the risk of TFF compared to conventional IVF in certain NMFI populations, such as unexplained infertility.⁸ However, a comprehensive meta-analysis indicated that the observed reduction in TFF with ICSI was predominantly seen in sibling oocyte studies and not consistently in patient-randomized trials.⁸ This meta-analysis also found that while FR per oocyte inseminated or injected was higher for ICSI, the FR per oocyte retrieved was similar between the two methods overall.⁸ This distinction is important: ICSI ensures sperm entry into mature oocytes selected for injection, potentially inflating FR per injected oocyte, whereas conventional IVF exposes all retrieved (mature and potentially some immature that mature in vitro) oocytes to sperm, and FR per retrieved oocyte reflects the overall cohort's fertilizability.
For instance, one large population-based study found that conventional IVF actually had a higher FR per oocyte retrieved than ICSI in NMFI cases (59.8% vs 56.2%).⁵³ Conversely, another study focusing on older women with low oocyte yield reported a higher normal fertilization rate with ICSI.⁴¹ While a different study on poor and suboptimal responders showed a higher 2PN fertilization rate with ICSI irrespective of oocyte number, yet better clinical outcomes with conventional IVF.⁴⁵ In PGT cycles using frozen-thawed embryos, fertilization method (conventional IVF vs. ICSI prior to freezing) did not impact subsequent PGT-A results or euploidy rates, implying comparable initial fertilization efficacy leading to viable blastocysts.⁴⁷
The inconsistency in FR benefits for ICSI in unselected NMFI, and the critical influence of the specific metric used (FR per oocyte retrieved vs. per oocyte inseminated/injected) and study design (sibling oocytes vs. patient randomization), suggests that an apparent increase in FR with ICSI does not automatically equate to a superior clinical strategy for all NMFI cases.
5.2. Embryo Quality, Cleavage, and Blastulation Rates
The impact of ICSI versus conventional IVF on subsequent embryo quality and development is not definitively established and appears to vary with patient populations and study methodologies. Some studies have reported higher rates of good quality embryos on day 2 or day 3 with ICSI in NMFI cohorts.⁵⁰ For example, a retrospective analysis of half-ICSI treatments found significantly higher 2PN rates and high-quality embryo rates with ICSI compared to IVF overall and in primary infertility patients.⁵⁰
However, other research presents a more nuanced or even contradictory picture. There are reports suggesting that ICSI might be associated with lower blastulation rates compared to conventional IVF in certain contexts, even if early embryo quality appears similar or better.⁵⁰⁺⁵² For poor responder patients with only a single oocyte retrieved, one study found similar rates of embryo formation and good quality embryos across groups treated with conventional IVF for NMFI, ICSI for NMFI, and ICSI for male factor infertility.⁵⁴ In PGT-A cycles utilizing frozen-thawed embryos, no significant differences were observed in blastocyst quality or development rates between embryos initially fertilized by conventional IVF versus ICSI.⁴⁷
A particularly concerning finding comes from a study that reported significantly lower euploidy rates and correspondingly higher aneuploidy rates in embryos derived from ICSI in non-male factor cases compared to both conventional IVF in NMFI and ICSI in male factor cases.⁵⁵ This suggests that the ICSI procedure itself, or the bypassing of natural selection mechanisms, might negatively impact chromosomal competence in oocytes that are not already challenged by severe sperm defects. However, this finding is not universal, as the PGT-A study on frozen-thawed embryos showed no difference in euploidy rates based on the initial fertilization method.⁴⁷
The data on embryo quality and blastulation remain inconsistent. While ICSI might sometimes result in a higher number of fertilized oocytes or embryos graded as good quality at early cleavage stages, this does not consistently translate into superior blastocyst development or, crucially, better euploidy rates, especially in NMFI. The potential for lower euploidy with NMFI-ICSI is a significant concern that warrants further rigorous investigation, as it implies that simply achieving fertilization does not guarantee a healthy embryo, and the intervention itself could have subtle detrimental effects on subsequent embryonic development in certain oocyte populations.
5.3. Implantation Rates (IR)
Implantation rate, the proportion of transferred embryos that successfully implant in the uterine lining, is a critical determinant of ART success. Evidence comparing IR between ICSI and conventional IVF in NMFI is varied. Several meta-analyses and large studies have suggested that ICSI may be associated with lower implantation rates compared to conventional IVF in NMFI populations.³⁸ For example, one meta-analysis reported a statistically significant better IR with IVF than with ICSI in NMFI.³⁸ Similarly, a large study focusing on poor and suboptimal ovarian responders found consistently higher IR with conventional IVF across different oocyte retrieval numbers (1–3, 4–6, 7–9 oocytes).⁴⁵
Conversely, other studies have not found significant differences in IR. For instance, in poor responder patients who had only a single oocyte retrieved, IRs were comparable between conventional IVF/NMFI, ICSI/NMFI, and ICSI/MFI groups.⁵⁴ In women with endometriosis but no male factor, IRs were also similar between IVF and ICSI derived embryos in a study where sibling oocytes were randomized.⁵²
If IR is indeed lower with ICSI in some NMFI cohorts, it would imply that even if an embryo is successfully created via ICSI and appears morphologically normal, its intrinsic viability or its ability to successfully engage in the complex dialogue required for implantation with the endometrium might be compromised compared to embryos derived from conventional IVF in these specific patient populations. This could be due to subtle, unobservable damages or alterations induced by the ICSI procedure, or due to the bypassing of natural selection processes that might normally filter out less competent gametes even before fertilization.
5.4. Clinical Pregnancy Rates (CPR)
Clinical pregnancy rate, defined as a pregnancy confirmed by ultrasound (typically showing a gestational sac with a fetal heartbeat), is a more robust indicator of ART success than fertilization or implantation rates alone. For NMFI, the overwhelming body of evidence, including RCTs, large cohort studies, and meta-analyses, indicates that ICSI does not offer an improvement in CPR compared to conventional IVF.⁴ In fact, some studies have even suggested similar or potentially lower CPR with ICSI in certain NMFI subgroups.
A meta-analysis focusing on NMFI found no significant difference in CPR between ICSI and conventional IVF.⁸ The study on poor and suboptimal ovarian responders reported significantly higher CPR with conventional IVF compared to ICSI.⁴⁵ For couples with unexplained infertility, one study found similar CPRs (50% in each group).³¹ While another reported higher CPR with IVF (35.2% vs 33.3% for ICSI, though not statistically significant).³⁹ When using cryopreserved-thawed embryos, CPRs were found to be similar regardless of whether the embryos were initially derived from conventional IVF or ICSI.⁴⁸ Similarly, in PGT-A cycles using frozen-thawed embryos, CPRs were comparable between the two fertilization methods.⁴⁷
The general lack of CPR improvement with ICSI in NMFI, despite occasional reports of higher fertilization rates, reinforces the understanding that successful fertilization is only one of many critical steps towards achieving a clinical pregnancy. Post-fertilization factors, including intrinsic embryo viability and endometrial receptivity, play crucial roles and are not necessarily enhanced, and could potentially be subtly impaired, by the ICSI procedure in oocytes from NMFI patients.
5.5. Live Birth Rates (LBR)
Live birth rate (LBR) is the ultimate and most important endpoint for couples undergoing infertility treatment and for evaluating the true efficacy of ART interventions. Regarding the comparison of ICSI and conventional IVF in NMFI, the evidence is remarkably consistent: ICSI does not improve LBR in unselected NMFI populations.⁴ This conclusion is supported by numerous RCTs, large-scale population-based cohort studies, and systematic reviews with meta-analyses.
For example, a large population-based study found the overall cumulative LBR to be 37.0% for conventional IVF and 36.0% for ICSI, with no significant difference in the likelihood of live birth for women undergoing ICSI compared to IVF in NMFI cases (Adjusted Hazard Ratio: 0.96).⁵³ Another meta-analysis confirmed no significant difference in LBR between ICSI and IVF in NMFI (RR 1.11, 95% CI 0.94 to 1.30).⁴ Some studies have even suggested a trend towards, or a statistically significant, lower LBR with ICSI in specific NMFI subgroups, such as women with tubal ligation only.⁵⁹ Or poor/suboptimal ovarian responders.⁴⁵ Professional guidelines from ASRM and other bodies reflect this lack of LBR benefit for the routine application of ICSI in NMFI.³¹ Even when considering cryopreserved-thawed embryos, LBRs have been found to be similar whether the embryos were originally created via conventional IVF or ICSI.⁴⁸
This consistent finding across various study designs and patient populations is the most compelling argument against the routine or widespread use of ICSI for NMFI. If the more invasive and costly procedure of ICSI does not translate into a higher chance of taking home a baby for these couples, its application in such scenarios warrants careful scrutiny and justification based on highly specific circumstances rather than broad diagnostic categories.
5.6. Outcomes in Severe Male Factor Infertility (SMFI)
In stark contrast to NMFI, ICSI is the undisputed treatment of choice for severe male factor infertility and has profoundly improved outcomes for this group. It effectively bypasses the severe deficiencies in sperm count, motility, morphology, or function that preclude fertilization with conventional IVF, enabling biological fatherhood for many men who would otherwise have no options or would have to resort to donor sperm.³
Fertilization rates with ICSI in SMFI cases are generally high. For instance, in a study of men with non-obstructive azoospermia (NOA) undergoing micro-TESE for sperm retrieval followed by ICSI, the fertilization rate was reported as 69.85%.³⁰ Live birth rates can also be substantial. The same study on NOA patients reported a cumulative LBR of 46.82% per couple once sperm were successfully retrieved and used for ICSI.³⁰ Another systematic review and meta-analysis focusing on testicular sperm for ICSI (T-ICSI) in men with high sperm DNA fragmentation or severe oligozoospermia found that T-ICSI led to significantly increased clinical pregnancy rates and LBRs, along with decreased miscarriage rates, compared to ICSI with ejaculated sperm in these specific challenging populations.²⁹
However, even within the SMFI category, success with ICSI is not universal and can be influenced by the specific underlying cause of the male infertility and concomitant female factors. For example, men with NOA due to AZFc microdeletions on the Y chromosome have been shown to have poorer embryological outcomes and lower cumulative LBR with ICSI compared to NOA from other causes.³⁰ Similarly, the actual number of sperm retrieved in azoospermic cases can impact success, with lower sperm counts retrieved being associated with lower LBR.³⁰ This highlights that while ICSI is a powerful tool to overcome the mechanical barrier of fertilization in SMFI, the intrinsic quality of the sperm (genetic and epigenetic) and oocyte factors still play a significant role in determining the ultimate success of the ART cycle.
5.7. Outcomes in Non-Male Factor Infertility (Subgroup Analyses where data permits)
Synthesizing the data from the preceding sections (5.1–5.5) specifically for NMFI, a consistent pattern emerges: while ICSI may, in some studies or subgroups, show an increase in fertilization rate per injected oocyte or a reduction in TFF (though the latter is debated based on study design), these intermediate benefits rarely translate into improved implantation rates, clinical pregnancy rates, or, most critically, live birth rates compared to conventional IVF.
For instance, in women with endometriosis but no coexisting male factor, conventional IVF has been shown to perform well, with cumulative clinical pregnancy and live birth rates similar to controls without endometriosis, suggesting ICSI is not routinely needed unless a male factor is also involved or there has been previous fertilization failure with IVF.⁴⁹ As discussed, for unexplained infertility, advanced maternal age, and poor ovarian response/low oocyte yield, robust evidence supporting a LBR advantage for ICSI is lacking, and in some cases, particularly for POR, conventional IVF may even yield better LBR.³¹ The only NMFI scenario where ICSI is broadly supported is following a documented failure or very poor fertilization with conventional IVF in a prior cycle.³¹ The overarching theme is that for most NMFI indications, ICSI does not offer a significant advantage in the most crucial patient-centered outcome – having a baby – over well-performed conventional IVF. Therefore, the decision to employ ICSI in NMFI should be highly selective and individualized, primarily reserved for cases with a clearly demonstrated or highly suspected issue with fertilization that ICSI can directly address.
Table 4: Meta-analysis Summary: Comparative Reproductive Outcomes (Fertilization Rate, Clinical Pregnancy Rate, Live Birth Rate) for Conventional IVF vs. ICSI in Key Patient Populations
Patient Population/Indication | Outcome Compared (ICSI vs. cIVF) | Pooled Effect Estimate (e.g., RR or OR with 95% CI) | Heterogeneity (I²) | General Conclusion from Meta-analyses | Key Reference(s) |
Severe Male Factor Infertility (SMFI) | Fertilization Rate (FR) | ICSI significantly higher than cIVF (cIVF often fails) | N/A (ICSI is standard) | ICSI is superior/necessary | 3 |
Live Birth Rate (LBR) | ICSI enables LBR where cIVF would likely fail | N/A (ICSI is standard) | ICSI enables LBR | 29 | |
Non-Male Factor Infertility (General/Unselected) | Fertilization Rate (per oocyte retrieved) | RR ≈ 1.05 (0.98–1.13) | High (92%) | No significant difference overall | 8 |
Fertilization Rate (per oocyte inseminated/injected) | RR ≈ 1.14 (1.08–1.20) | Moderate (69%) | ICSI higher | 8 | |
Total Fertilization Failure (TFF) | RR ≈ 0.26 (0.13–0.50) overall; RR ≈ 0.72 (0.48–1.06) in patient-randomized studies | Moderate (58%) overall; Low (0%) in patient-randomized | ICSI reduces TFF in sibling oocyte studies; no significant difference in patient-randomized studies | 8 | |
Clinical Pregnancy Rate (CPR) | RR ≈ 1.04 (0.66–1.64) in RCTs; RR ≈ 0.85 (0.77–0.94) in cohort studies (IVF higher) | N/A for RCTs; N/A for Cohorts | No advantage or IVF better | 57 | |
Live Birth Rate (LBR) | RR ≈ 1.11 (0.94–1.30) (3 RCTs); RR ≈ 0.86 (0.79–0.94) in cohort studies (IVF higher) | Low (0%) for RCTs; N/A for Cohorts | No advantage or IVF better | 4 | |
Unexplained Infertility | Fertilization Rate | RR ≈ 0.99 (0.90–1.09) | N/A | No significant difference | 38 |
Implantation Rate | RR ≈ 0.77 (0.64–0.93) (IVF higher) | N/A | IVF better | 38 | |
Live Birth Rate (Fresh ET) | RR ≈ 0.89 (0.77–1.03) | N/A | No significant difference overall; IVF better if AMA >35 | 38 | |
Advanced Maternal Age (>35 or >38 years) | Live Birth Rate | Generally no improvement with ICSI | N/A | No benefit from ICSI | 31 |
Poor Ovarian Responders / Low Oocyte Yield | Live Birth Rate | No improvement or potentially lower with ICSI | N/A | No benefit, cIVF may be better | 31 |
N/A: Not applicable if ICSI is standard or data not directly comparable from cited meta-analyses in this format. RR = Relative Risk; OR = Odds Ratio; CI = Confidence Interval. Conclusions are generalized from the cited sources.
6. Safety and Risks
The safety of ART procedures, for both the mother and the resulting offspring, is a paramount concern. This section examines potential risks associated with conventional IVF and ICSI.
6.1. Maternal Complications
Maternal complications in ART are generally related to the processes of controlled ovarian stimulation and oocyte retrieval, rather than the specific method of fertilization (conventional IVF versus ICSI).⁶⁰ Key risks include:
Ovarian Hyperstimulation Syndrome (OHSS): This is a potentially serious complication of COS, characterized by enlarged ovaries, fluid accumulation in the abdomen, and other systemic effects. Modern stimulation protocols, including the use of GnRH antagonists and agonist triggers, aim to minimize this risk.⁶¹
Risks of Egg Retrieval: This surgical procedure carries small risks of bleeding, infection, and injury to pelvic organs, as well as risks associated with anesthesia.⁶²
Multiple Pregnancies: ART, historically, has been associated with a higher rate of multiple pregnancies (twins, triplets, etc.), which carry increased risks for both mother (e.g., preeclampsia, gestational diabetes, cesarean delivery) and babies (e.g., prematurity, low birth weight). The increasing adoption of elective single embryo transfer (eSET) strategies is aimed at reducing this risk.⁴⁶
Ectopic Pregnancy: While uncommon, the risk of ectopic pregnancy may be slightly elevated after ART.
Ovarian Torsion: Enlarged ovaries due to stimulation can occasionally twist, requiring emergency intervention.
The available research does not strongly differentiate these maternal risks specifically between conventional IVF and ICSI cycles, suggesting they are more broadly linked to the overall ART process common to both.
6.2. Offspring Health: Congenital Anomalies and Birth Defects
The health of children conceived via ART has been extensively studied. It is generally accepted that ART-conceived children (from both IVF and ICSI) have a slightly higher risk of certain congenital anomalies compared to children conceived naturally.⁴ This overall increased risk is estimated to be around 30–40% higher than in the general population, though the absolute risk remains relatively low (e.g., increasing from ~3% to ~4–5%). It is important to note that some of this increased risk may be attributable to the underlying parental subfertility, advanced parental age, or other comorbidities common in couples seeking ART, rather than solely to the ART procedures themselves.⁶⁰
The specific question of whether ICSI carries an additional risk of birth defects compared to conventional IVF has been a subject of considerable debate with conflicting findings:
Studies Suggesting Increased Risk with ICSI: Some large cohort studies and meta-analyses have reported a slightly higher prevalence of major malformations in children conceived via ICSI compared to those conceived via conventional IVF.⁴ For example, analyses by Davies et al. (2012) and Luke et al. (2021) suggested such an association.⁴ An increased risk of hypospadias in male offspring has been specifically noted in some ICSI series, particularly when ICSI was used for male factor infertility, suggesting a link to paternal factors transmitted via ICSI.⁴ The ASRM 2020 committee opinion acknowledges these conflicting data but highlights studies indicating an increased risk with ICSI, thus warranting caution, especially for unindicated use.³¹
Studies Suggesting No Significant Additional Risk with ICSI: Conversely, other meta-analyses, such as one by Lie et al. (2005), which included four prospective cohort studies, found no statistically significant difference in the overall risk of major birth defects between children born after ICSI and those born after conventional IVF (pooled RR 1.12, 95% CI: 0.97–1.28).⁶⁵
The "ICSI Paradox": A central concept in this discussion is the "ICSI paradox".³ Conventional IVF allows for some degree of natural sperm selection, as sperm must be capable of motility, capacitation, and oocyte penetration. ICSI bypasses these natural selection mechanisms by allowing an embryologist to select a single sperm (often based on limited morphological criteria) and inject it directly into the oocyte. This may inadvertently facilitate the transmission of sperm with genetic or epigenetic defects that would normally be filtered out.
Disentangling the effects of the ICSI procedure from the underlying severe male infertility for which it is often indicated is a major methodological challenge. The slightly higher risk of certain anomalies observed in some ICSI cohorts might be linked to the paternal genetic or epigenetic background rather than the micromanipulation technique itself.
6.3. Offspring Health: Genetic and Epigenetic Concerns
The direct nature of ICSI raises specific concerns about the transmission of genetic and epigenetic abnormalities.
Genetic Risks:
Transmission of Paternal Defects: ICSI enables men with genetic conditions causing their infertility to father children, thereby transmitting these conditions. For example, men with Y-chromosome microdeletions (a cause of severe oligozoospermia or azoospermia) will pass these deletions to their male offspring, who will likely also experience infertility.²⁸ Similarly, men with congenital bilateral absence of the vas deferens (CBAVD) often have mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene; ICSI allows them to have children, but their offspring have an increased risk of inheriting CFTR mutations and potentially developing cystic fibrosis if the female partner is also a carrier.²⁸
Chromosomal Abnormalities: An increased prevalence of sex chromosome abnormalities (e.g., Klinefelter syndrome (47,XXY), Turner syndrome (45,X), 47,XYY) has been reported in children conceived via ICSI, with rates around 0.8–1.0% compared to approximately 0.2% in the general IVF population and 0.5–0.6% in naturally conceived newborns.¹⁶ De novo structural chromosomal abnormalities have also been reported at slightly higher rates.
Epigenetic Risks:
Epigenetic modifications (such as DNA methylation and histone modifications) are crucial for normal gene regulation and embryonic development. There are concerns that ART procedures, occurring during critical windows of epigenetic reprogramming in gametes and early embryos, might disrupt these patterns.³
Imprinting Disorders: Particular attention has been paid to genomic imprinting, an epigenetic process leading to parent-of-origin-specific gene expression. Several rare imprinting disorders, such as Beckwith-Wiedemann syndrome (BWS), Angelman syndrome (AS), and Silver-Russell syndrome (SRS), have been reported at a higher frequency in children conceived via ART, including ICSI, compared to naturally conceived children.³ The absolute risk remains very low (less than 1% of ICSI-conceived children³), but the relative risk appears to be increased several-fold.
Contributing Factors: It is challenging to determine whether these epigenetic alterations are caused by the underlying parental subfertility (as sperm from infertile men can have aberrant epigenetic marks), ovarian stimulation protocols, in vitro embryo culture conditions (media composition, oxygen tension), or the ICSI procedure itself (e.g., injection of immature sperm or bypassing natural oocyte activation signals).²⁸ Some research suggests that certain DNA methylation differences observed in ART infants may largely resolve by adulthood, but the long-term significance of subtle epigenetic variations is still an area of active investigation.⁶⁰
ICSI’s inherent mechanism of bypassing natural selection means it carries a tangible risk of transmitting known paternal genetic defects. Epigenetic concerns are more complex and likely multifactorial, involving the entire ART process, but the direct manipulation of gametes in ICSI places it under particular scrutiny.
6.4. Offspring Health: Neurodevelopmental Outcomes and Long-Term Health
The long-term health and neurodevelopmental outcomes of children conceived via ART, and specifically ICSI, are of significant interest and ongoing research.
Neurodevelopmental Outcomes:
Early studies on the neurodevelopmental outcomes of ICSI children yielded conflicting results, with some suggesting potential delays. However, more recent and larger studies, particularly those employing robust methodologies like causal inference analysis and appropriate control groups, are increasingly reassuring. A significant population-based study found no causal effect of ICSI (for non-severe male factor infertility) on the risk of AEDC-defined developmental vulnerability at school-entry age compared with children conceived via standard IVF.⁶⁶
Concerns about increased risks of autism spectrum disorder (ASD) or intellectual disability with ICSI have been raised by some studies.⁷ However, this association is not consistently found across all research and may be confounded by factors such as parental characteristics, underlying infertility diagnoses, or increased surveillance in ART populations. The ASRM notes that the safety of ICSI for non-male factor infertility has not been fully evaluated in this regard.³¹
Long-Term General Health:
Studies investigating various aspects of long-term health in ART/ICSI offspring, including cardiometabolic profiles (blood pressure, cholesterol, glucose metabolism), respiratory health (asthma, allergies), thyroid function, and cancer risk, have produced mixed results.⁶⁰ While some earlier or smaller studies indicated minor differences in certain parameters (e.g., slightly higher blood pressure), many larger, well-controlled follow-up studies extending into adolescence and young adulthood have found largely reassuring outcomes, with ART-conceived individuals generally falling within normal physiological ranges and often comparable to naturally conceived peers, especially after adjusting for perinatal factors like prematurity or low birth weight.
Hospitalization rates for ART-conceived children may be slightly higher than for naturally conceived children, but this could be influenced by increased parental vigilance or underlying parental health factors rather than the ART procedure itself.⁶⁰
A theoretical concern, particularly for males conceived via ICSI due to paternal SMFI, is their future fertility. If the father's infertility has a genetic basis (e.g., Y-chromosome microdeletion), it is likely to be transmitted to his sons.²⁸ Long-term follow-up studies into adulthood are beginning to emerge, with some studies on young men conceived by IVF/ICSI showing generally reassuring testicular function but subtle differences in some semen parameters or hormone levels compared to spontaneously conceived men.⁶⁷
While initial concerns about long-term outcomes were significant, the evolving body of evidence, particularly from larger and better-controlled studies, tends to be more reassuring regarding major adverse health or neurodevelopmental consequences specifically attributable to ICSI compared to conventional IVF, especially when parental subfertility is accounted for. Nevertheless, ART is a relatively young field in terms of tracking multi-generational health, and continued long-term surveillance of ART-conceived individuals is warranted.
Table 5: Summary of Potential Risks and Safety Concerns for Mother and Offspring: Conventional IVF vs. ICSI
Risk Category | Specific Concern | Conventional IVF | ICSI | Notes / Level of Evidence | Reference(s) |
Maternal | Ovarian Hyperstimulation Syndrome (OHSS) | Yes (related to COS) | Yes (related to COS) | Risk associated with ovarian stimulation, not fertilization method. | 61 |
Egg Retrieval Complications (bleeding, infection) | Yes | Yes | Procedural risk, not specific to fertilization method. | 62 | |
Multiple Pregnancy | Yes (if multiple embryos transferred) | Yes (if multiple embryos transferred) | Related to embryo transfer practice, reduced by eSET. | 61 | |
Offspring (General ART vs. Natural Conception) | Overall Congenital Anomalies | Slightly Increased Risk | Slightly Increased Risk (potentially higher than cIVF in some studies) | ART overall has ~30-40% higher relative risk vs. natural. Absolute risk low. | 4 |
Preterm Birth / Low Birth Weight | Increased Risk | Increased Risk | Common ART outcome, multifactorial. | 60 | |
Offspring (ICSI vs. Conventional IVF) | Major Congenital Anomalies (Overall) | Baseline ART Risk | Conflicting: Some studies suggest slightly higher risk, others no significant difference vs. cIVF. | Evidence is mixed; difficult to separate procedure from underlying MFI. | 22 |
Specific Anomalies (e.g., Hypospadias) | Baseline ART Risk | Potentially higher risk, especially if MFI is indication. | Some evidence for increased hypospadias. | 4 | |
Genetic Transmission (Paternal) | Lower risk (natural selection in vitro) | Higher risk (e.g., Y-microdeletions, CFTR mutations with CBAVD) due to bypassing natural selection. | Established risk for known paternal genetic conditions. | 3 | |
Sex Chromosome Abnormalities | Baseline ART Risk | Increased prevalence reported (0.8-1.0%). | Consistent finding in several studies. | 16 | |
Epigenetic Risks (Imprinting Disorders) | Potential Risk (ART-related) | Potential Risk (ART-related, possibly higher due to manipulation/sperm source). | Increased relative risk for rare disorders like BWS, AS. Absolute risk low. Multifactorial. | 3 | |
Neurodevelopmental Outcomes (School Age) | Baseline ART Risk | Generally no significant difference vs. cIVF in recent large studies for non-severe MFI. Earlier concerns about ASD/ID not consistently confirmed. | Reassuring data emerging, but long-term surveillance ongoing. | 53 | |
Oocyte Damage | Minimal/Indirect | Direct physical penetration; low risk (5-10%) with experienced embryologists. | Inherent to ICSI procedure. | 16 |
7. Economic Considerations
The economic aspects of choosing between conventional IVF and ICSI are significant, impacting patients, healthcare providers, and healthcare systems. These considerations involve not only the direct costs of the procedures but also their cost-effectiveness in achieving the desired outcome of a live birth.
7.1. Cost-Effectiveness Analysis: ICSI vs. Conventional IVF
ICSI is consistently reported to be more expensive than conventional IVF. This increased cost is attributed to the additional laboratory labor involved in oocyte denudation, sperm selection, and the micromanipulation procedure itself, as well as the specialized equipment and consumables required.²² Estimates of this additional cost vary by region and healthcare system; for example, around A$600–A$624 per cycle in Australia in the early 2000s⁶⁸, an 8.3% higher cost in some Dutch centers³², or an additional charge of approximately $1,500 in the United States.⁴⁶
The cost-effectiveness of ICSI is highly dependent on the clinical indication:
Severe Male Factor Infertility (SMFI): In cases of SMFI where conventional IVF has a very low or negligible chance of success, ICSI is generally considered cost-effective. It provides a pathway to achieving fertilization and live birth that would otherwise be unavailable.⁶⁸ For patients entirely unsuited to conventional IVF, the incremental cost per live birth achieved with ICSI can range from approximately A$8,500 to A$13,400. For subnormal semen parameters where IVF might still offer some chance, the incremental cost per additional live birth with ICSI could be as low as A$3,600 if it significantly improves LBR, but could also represent an additional cost with no benefit if LBR is not improved.⁶⁸
Non-Male Factor Infertility (NMFI): For NMFI, where conventional IVF is a viable option and LBRs are generally comparable to ICSI (as discussed in Section 5.5), the routine use of ICSI is typically not cost-effective.³² The additional cost of ICSI does not translate into a higher likelihood of live birth for these patients. One older UK-based estimate suggested an incremental cost of £60,000 (approximately A$152,400 at the time) to gain one additional live birth if ICSI were advocated for all IVF patients, assuming only a very small LBR advantage for ICSI.⁶⁸ A recent systematic review of economic evaluations concluded that ICSI for unexplained infertility is unlikely to be cost-effective due to minimal or no increase in effectiveness (LBR).⁷⁰ However, the same review noted that “rescue ICSI” (performed on oocytes that failed to fertilize with conventional IVF on Day 1) might be cost-effective as an alternative to cycle cancellation in those specific circumstances.⁷⁰
Willingness-to-pay thresholds are often considered in cost-effectiveness analyses. For example, if the cost to achieve one live birth via a standard ART cycle for a 30-year-old woman is estimated at around $27,000 in the US, interventions that cost significantly more than this per additional live birth gained may be considered not cost-effective.⁷¹ For NMFI, the marginal or absent improvement in LBR with ICSI means its incremental cost-effectiveness ratio often exceeds such thresholds. The crucial determinant of ICSI’s cost-effectiveness is its ability to improve LBR over conventional IVF for a given indication; for SMFI, this improvement is substantial, whereas for most NMFI cases, it is not.
7.2. Financial Implications of Routine ICSI Use for Patients and Healthcare Systems
The routine or widespread use of ICSI, particularly in NMFI cases where its benefit is not established, has significant financial implications. It substantially increases the overall cost of ART for individual patients, who often bear these costs out-of-pocket, and for healthcare systems if ART is publicly funded or subsidized.⁷
The cumulative financial burden of non-indicated ICSI can be considerable. An older Australian estimate suggested that the overuse of ICSI could add over A$31 million per annum to national ART expenditures.⁶⁸ Such increased expenditure on a procedure without proven superior outcomes in many common scenarios raises important questions about the responsible stewardship of healthcare resources and the potential for misallocation.
Furthermore, the cost of ART can be a significant barrier to access for many individuals and couples. The introduction of patient co-payments or increased out-of-pocket expenses for procedures like ICSI can reduce the demand for ART services, highlighting a degree of price elasticity in this area of healthcare.⁷² This can exacerbate inequities in access to fertility treatment, potentially limiting options for those with fewer financial resources.⁷² The common practice of planning ART on a cycle-by-cycle basis may also obscure the long-term financial commitment from patients, who might not fully appreciate the cumulative costs if multiple cycles are needed, especially if a more expensive, non-indicated procedure like ICSI is chosen from the outset.⁷⁴ This underscores the importance of transparent counseling regarding not only the clinical but also the financial aspects of different treatment options.
Table 6: Cost-Effectiveness Comparison: ICSI vs. Conventional IVF in Different Scenarios (Illustrative Data)
Scenario / Indication | Additional Cost per ICSI Cycle (approx.) | Incremental Cost per Additional Live Birth with ICSI (vs. cIVF or no treatment) | Cost-Effective? | Key Reference(s) |
Severe Male Factor Infertility (SMFI) (Patient unsuited to cIVF) | A$600 - $1,500 (USD) + potential surgical sperm retrieval costs | A$8,500 – A$13,400 (vs. no treatment) <br> US$32,869 (vs. IUI, older data) | Generally Yes (provides chance of LBR vs. none/low) | 46 |
Subnormal Semen (cIVF possible but suboptimal) | A$600 - $1,500 (USD) | A$3,600 (best case) to Dominated (worst case, no LBR gain) | Variable (depends on LBR gain over cIVF) | 68 |
Non-Male Factor Infertility (NMFI) / Unexplained Infertility (Routine Use) | A$600 - $1,500 (USD) | Very High (e.g., £60,000 / A$152,400 for 1% LBR gain) or Dominated (if no LBR gain) | Generally No (due to lack of LBR improvement over cIVF) | 32 |
Rescue ICSI (after TFF with cIVF) | Cost of ICSI procedure | Potentially lower overall cost than cycle cancellation and restart. | May be Yes (avoids cost of failed cycle/restart) | 70 |
Costs are illustrative and vary significantly by region, clinic, and year. "Dominated" means higher cost for no additional benefit or worse outcome. Data often from different time periods and healthcare systems.
8. Ethical Considerations and Professional Guidelines
The application of ART, particularly the choice between conventional IVF and ICSI, involves significant ethical considerations related to patient autonomy, beneficence, non-maleficence, justice (resource allocation), and adherence to evidence-based medicine. Professional guidelines from bodies like ASRM, ESHRE, and NICE play a crucial role in navigating these complexities.
8.1. The Debate on Routine ICSI for Non-Male Factor Infertility
The widespread and increasing use of ICSI for NMFI, despite a general lack of evidence for improved LBR in many of these scenarios, is a focal point of ethical debate.⁷
Medicalization and Best Interest: Performing a more invasive and costly procedure without clear benefit raises questions about whether it truly serves the patient's best interest or contributes to unnecessary medicalization of infertility treatment.
Evidence-Based Practice: The principle of evidence-based medicine dictates that clinical decisions should be grounded in the best available scientific evidence. The routine use of ICSI for NMFI often falls short of this standard when LBR is the primary outcome measure.
Avoiding Total Fertilization Failure (TFF): A common justification for using ICSI in NMFI is to prevent the distressing outcome of TFF that can occur in a small percentage of conventional IVF cycles.⁷ While reducing TFF is a desirable intermediate outcome, it must be weighed against the lack of LBR improvement, the additional costs, and any potential risks associated with ICSI. The number needed to treat (NNT) with ICSI to prevent one case of TFF in NMFI is reportedly high (e.g., 33 couples according to an ASRM-cited study³¹), suggesting that many couples undergo the procedure without benefiting from this specific risk reduction.
The "ICSI Paradox" and Non-Maleficence: The concern that ICSI bypasses natural sperm selection mechanisms, potentially allowing the transmission of sperm with genetic or epigenetic defects, relates to the ethical principle of non-maleficence (do no harm).³ If ICSI is used without a strong indication, it may expose the oocyte and resulting embryo/offspring to these potential risks unnecessarily.
8.2. Resource Allocation and Justice
The higher cost of ICSI compared to conventional IVF has significant implications for resource allocation, both at the individual patient level and for the broader healthcare system.²²
Individual Burden: For patients paying out-of-pocket, the additional cost of ICSI can be substantial, potentially limiting access to treatment or reducing the number of cycles they can afford, especially if ICSI is used routinely without clear benefit.³²
Societal Burden: In healthcare systems with public funding or insurance mandates for ART, the routine use of ICSI for NMFI diverts resources towards a more expensive procedure that may not offer superior outcomes, potentially at the expense of other needed healthcare services or limiting the number of publicly funded cycles available.
Equity of Access: Disparities in insurance coverage and the ability to pay can lead to inequitable access to ART. The promotion of more expensive, non-indicated procedures can exacerbate these inequities.⁷² Ethical considerations of justice demand that resources be allocated fairly and efficiently to maximize health benefits for the population.
8.3. Patient Autonomy and Informed Consent
Respect for patient autonomy is a cornerstone of medical ethics, requiring that patients make voluntary, informed decisions about their medical care.
Full Disclosure: Patients should receive comprehensive, unbiased information about the proposed treatment options (conventional IVF and ICSI), including their respective rationales, procedures, potential benefits (especially LBR), risks (for mother and offspring), alternatives (including no treatment or other ART options), and costs.³³ This includes discussing the uncertainties and controversies, particularly regarding ICSI for NMFI.
Understanding Complex Information: The complexity of ART procedures and the nuances of statistical outcomes can make it challenging for patients to fully grasp the information provided.⁷⁵ Clinicians have an ethical duty to facilitate understanding, using clear language and decision aids if helpful.
Shared Decision-Making: The decision to use ICSI, especially in NMFI cases, should be a shared one between the clinician and the patient/couple, based on their individual circumstances, values, and understanding of the evidence.⁷⁶
Pressure and Vulnerability: Patients seeking fertility treatment are often in a vulnerable emotional state, which can impact their decision-making. Clinicians must be mindful of avoiding undue pressure or creating unrealistic expectations.⁷⁵
8.4. Professional Guidelines (ASRM, ESHRE, NICE)
Major reproductive medicine societies provide guidance on the appropriate use of ICSI:
ASRM (American Society for Reproductive Medicine): ASRM committee opinions generally advise against the routine use of ICSI for NMFI where LBR is not improved. They support ICSI for severe MFI, previous fertilization failure with conventional IVF, and in specific situations like PGT for monogenic diseases (if contamination is a risk) or with cryopreserved oocytes. They emphasize considering the additional cost and lack of LBR benefit for many NMFI indications.⁴
ESHRE (European Society of Human Reproduction and Embryology): ESHRE guidelines also tend to be conservative regarding ICSI for NMFI, advising against its routine use in such cases.²² Their focus is on evidence-based indications.
NICE (National Institute for Health and Care Excellence, UK): NICE guidelines recommend that ICSI be offered only if there are severe deficits in semen quality, obstructive or non-obstructive azoospermia, or if previous IVF treatment resulted in failed or very poor fertilization.³³ They emphasize that while ICSI may increase fertilization chances in these specific scenarios, it does not necessarily improve the chance of a successful pregnancy beyond that.
These guidelines underscore the importance of adhering to evidence-based indications for ICSI and highlight the ethical responsibility of clinics to justify their use of ICSI, particularly in NMFI cases. The gap between these guidelines and the widespread clinical practice of routine ICSI in many regions remains a significant ethical challenge.³³
9. Patient Counseling and Informed Consent
Effective patient counseling and a robust informed consent process are critical when patients are considering ART, particularly when choosing between conventional IVF and ICSI. This process must be tailored to the individual couple's specific circumstances, diagnosis, and treatment history.
Key elements of counseling and informed consent should include:
Clear Explanation of Procedures: A detailed explanation of both conventional IVF and ICSI procedures, highlighting the differences in how fertilization is achieved in the laboratory.³³ This should cover oocyte retrieval, sperm preparation, the insemination/injection process, embryo culture, and embryo transfer.
Indications for Each Technique: A clear discussion of why one technique might be recommended over the other based on the couple's specific infertility diagnosis. This includes explaining the strong indications for ICSI in cases of severe male factor infertility or previous fertilization failure with IVF, and the lack of established benefit for many non-male factor indications.³³
Success Rates: Presentation of realistic and individualized success rates, focusing primarily on live birth rates per cycle started or per embryo transfer. It is important to differentiate between intermediate outcomes (like fertilization rates, which may be higher with ICSI in some NMFI scenarios) and the ultimate outcome of a healthy baby.⁶² Patients should be informed that for most NMFI, ICSI does not improve LBR over conventional IVF.³¹
Risks and Benefits: A balanced discussion of the potential benefits and risks associated with each procedure for both the woman undergoing treatment and any resulting offspring.
Maternal Risks: Risks common to all ART cycles (OHSS, procedural risks from egg retrieval, multiple pregnancy if more than one embryo is transferred) should be covered.⁶²
Offspring Risks: This should include the general slightly increased risk of congenital anomalies with ART compared to natural conception. Specific to ICSI, the discussion should cover the conflicting evidence regarding a potential additional risk of birth defects compared to conventional IVF, the established risk of transmitting paternal genetic conditions (e.g., Y-chromosome microdeletions, CFTR mutations in CBAVD), the slightly increased risk of sex chromosome abnormalities, and the theoretical (though generally low absolute risk) concerns about epigenetic alterations and imprinting disorders.¹⁶ The current understanding of long-term neurodevelopmental outcomes (largely reassuring for ICSI vs. IVF in NMFI) should also be presented.⁶⁶
Alternatives: Discussion of all reasonable alternatives, including less invasive treatments (if applicable), using donor gametes, adoption, or choosing not to pursue treatment.⁶²
Costs: Transparent information about the costs of conventional IVF versus ICSI, including any additional fees for ICSI, and the overall financial commitment involved in ART treatment, which may require multiple cycles.³²
Uncertainties: Acknowledgment of areas where evidence is limited or conflicting, and any unknown long-term effects.⁶²
Emotional and Psychological Aspects: Acknowledging the emotional stress of infertility and ART, and offering resources for psychological support.
Opportunity for Questions: Ensuring patients have ample opportunity to ask questions and have them answered satisfactorily before making a decision.⁶²
The ASRM Ethics Committee emphasizes a shared decision-making model, where the patient is supported in understanding their medical options and making a voluntary, autonomous decision.⁷⁶ Given the "overuse" of ICSI in non-male factor infertility and the gap between clinical practice and evidence-based guidelines,³³ it is particularly important that counseling for NMFI couples clearly outlines the lack of proven LBR benefit with ICSI and its additional costs and potential risks, allowing them to make a truly informed choice.
10. Future Directions
Despite decades of research and clinical application, several areas concerning conventional IVF and ICSI warrant further investigation to refine clinical practice and improve patient outcomes:
Long-Term Health of ICSI Offspring in NMFI: While current data on neurodevelopmental and general health outcomes for ICSI children (especially compared to IVF children in NMFI settings) are largely reassuring into adolescence,⁶⁶ truly long-term (adult and multi-generational) follow-up studies are still needed to definitively assess any subtle, late-onset effects, particularly concerning epigenetic modifications and future fertility.
Refining Indications for ICSI in NMFI: Further high-quality RCTs are needed to identify specific subgroups within NMFI (beyond previous IVF fertilization failure) who might genuinely benefit from ICSI in terms of LBR. This includes better understanding the mechanisms behind unexplained infertility and whether specific oocyte or sperm functional defects not captured by routine analyses could be overcome by ICSI.
Optimizing Sperm Selection for ICSI: The "ICSI paradox" highlights the limitations of current morphological sperm selection. Research into advanced sperm selection techniques (e.g., IMSI, microfluidics, QPM, functional sperm tests) needs to continue, with a focus on demonstrating clear improvements in LBR and offspring safety before widespread adoption.³ The development of non-invasive, objective methods for selecting functionally competent and genetically/epigenetically normal sperm is a key goal.
Understanding and Mitigating Epigenetic Risks: More research is needed to understand the specific impact of different ART components (ovarian stimulation, culture media, ICSI procedure itself) on the epigenome of gametes and embryos, and the long-term consequences for offspring health.²⁸ Identifying safer laboratory protocols could minimize these risks.
Cost-Effectiveness in Specific NMFI Subgroups: Rigorous economic evaluations are needed to assess the cost-effectiveness of ICSI in narrowly defined NMFI subgroups where a potential LBR benefit might be hypothesized or demonstrated, to ensure responsible resource allocation.
Improving Fertilization Assessment in Conventional IVF: Developing better predictors of TFF in conventional IVF could help to more accurately identify couples who would benefit from ICSI in their first cycle, rather than resorting to routine ICSI or experiencing a failed cycle.
Standardization of Practices and Reporting: Greater international standardization in ART laboratory practices, diagnostic criteria for male infertility, and reporting of outcomes would facilitate more robust comparisons and meta-analyses.
Addressing these areas will help to ensure that both conventional IVF and ICSI are used in the most effective, safe, and economically responsible manner, tailored to the specific needs of each infertile couple.
11. Conclusion
Conventional IVF and ICSI are transformative assisted reproductive technologies that have enabled millions to achieve parenthood. Conventional IVF, the foundational technique, remains a robust and effective treatment for a wide range of infertility causes where sperm are capable of fertilizing oocytes in vitro. ICSI, developed as a direct solution to severe male factor infertility, has undeniably revolutionized treatment for men with severely compromised sperm parameters or azoospermia, offering them a chance at biological fatherhood that was previously impossible. For this indication, ICSI is indispensable and its benefits clearly outweigh the additional procedural complexity and cost.
However, the landscape becomes considerably more complex with the widespread and increasing application of ICSI for non-male factor infertility. Despite its theoretical appeal for overcoming potential, often undefined, fertilization barriers or for maximizing oocyte utilization, the overwhelming body of evidence from large cohort studies, randomized controlled trials, and systematic reviews indicates that ICSI does not confer a significant advantage in live birth rates over conventional IVF for most NMFI indications. This includes unexplained infertility, advanced maternal age, and poor ovarian response. While ICSI may increase fertilization rates in some specific NMFI scenarios or reduce the incidence of total fertilization failure, these intermediate benefits do not consistently translate into more babies being born. The notable exception within NMFI is its utility following a documented previous cycle of failed or very poor fertilization with conventional IVF.
This "indication creep" for ICSI is concerning from several perspectives. It represents a departure from strictly evidence-based practice, incurs significant additional costs for patients and healthcare systems without a proportional improvement in the most crucial outcome, and exposes oocytes and embryos to a more invasive procedure that bypasses natural selection mechanisms, with ongoing (though often reassuring) surveillance of potential long-term offspring health implications, including subtle genetic and epigenetic concerns.
Professional guidelines from ASRM, ESHRE, and NICE consistently advocate for a more judicious use of ICSI, recommending it primarily for severe male factor infertility and previous IVF fertilization failure, and cautioning against its routine application in NMFI. Adherence to these guidelines, coupled with thorough and individualized patient counseling that transparently discusses the evidence regarding efficacy, risks, and costs, is paramount. Future research should continue to explore the long-term safety of ICSI, refine sperm selection techniques, and better identify the small subset of NMFI patients, if any, who might genuinely benefit from this intervention. Ultimately, the goal of ART is a healthy live birth, and the choice of fertilization method should be guided by the best available evidence to achieve this outcome in the safest and most cost-effective manner for each unique patient or couple.
Works cited
Understanding fertilization through intracytoplasmic sperm injection ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC4046257/
Assisted Reproductive Technology after the Birth of Louise Brown ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3799275/
'Intracytoplasmic sperm injection (ICSI) paradox' and 'andrological ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10863146/
Intracytoplasmic sperm injection versus conventional in vitro ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10426261/
ICSI Vs. IVF | Pacific Reproductive Center, accessed May 21, 2025, https://www.pacificreproductivecenter.com/what-are-the-differences-between-icsi-and-conventional-ivf/
Oocyte activation for women following intracytoplasmic sperm ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC8214070/
The Impact of Intracytoplasmic Sperm Injection in Non-Male Factor ..., accessed May 21, 2025, https://www.mdpi.com/2077-0383/10/12/2616
Efficacy of intracytoplasmic sperm injection in women with non‐male ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10755139/
Infertility & assisted reproduction: A historical & modern scientific ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC6469376/
ART: Step-by-Step Guide - Society for Assisted Reproductive Technology, accessed May 21, 2025, https://www.sart.org/patients/a-patients-guide-to-assisted-reproductive-technology/general-information/art-step-by-step-guide/
A Complete Step-by-Step Guide to the ICSI Procedure - Ferty9, accessed May 21, 2025, https://www.ferty9.com/blog/icsi-procedure-guide
The IVF Lab Process Explained at AFCC | Blog, accessed May 21, 2025, https://www.advancedfertility.com/blog/the-ivf-lab-process-explained
Swim-up versus density gradients for sperm preparation in infertile couples undergoing intrauterine insemination: a randomized clinical trial | Human Reproduction | Oxford Academic, accessed May 21, 2025, https://academic.oup.com/humrep/advance-article/doi/10.1093/humrep/deaf047/8093629?rss=1
swim-up and density gradient centrifugation - JaypeeDigital | eBook Reader, accessed May 21, 2025, https://www.jaypeedigital.com/eReader/chapter/9781907816468/ch5
Sperm Selection for ICSI by Morphology (Chapter 25) - Principles of IVF Laboratory Practice, accessed May 21, 2025, https://www.cambridge.org/core/books/principles-of-ivf-laboratory-practice/sperm-selection-for-icsi-by-morphology/F309D9737AA9B1AF0BA9090CBB7DD7C0
Intracytoplasmic sperm injection (ICSI) patient education fact sheet | ReproductiveFacts.org, accessed May 21, 2025, https://www.reproductivefacts.org/news-and-publications/fact-sheets-and-infographics/intracytoplasmic-sperm-injection-icsi/
Oocyte Denudation | American Society for Reproductive Medicine ..., accessed May 21, 2025, https://www.asrm.org/practice-guidance/coding-resources/coding/coding-art-lab-procedures/oocyte-denudation/
Stain-Free Sperm Analysis and Selection for Intracytoplasmic Sperm Injection Complying with WHO Strict Normal Criteria - MDPI, accessed May 21, 2025, https://www.mdpi.com/2227-9059/11/10/2614
SLM B-Series Holding Pipettes - Irvine Scientific, accessed May 21, 2025, https://www.irvinesci.com/slm-b-series-holding-pipettes.html
Holding Pipettes - Vitrolife, accessed May 21, 2025, https://www.vitrolife.com/products/micromanipulation-pipettes/holding-pipettes/
Fertility evaluation of infertile women: a committee opinion (2021) | American Society for Reproductive Medicine | ASRM, accessed May 21, 2025, https://www.asrm.org/practice-guidance/practice-committee-documents/fertility-evaluation-of-infertile-women-a-committee-opinion-2021/
Should I opt for intracytoplasmic sperm injection or should I not: high ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10958696/
The Sixth Edition of the WHO Manual for Human Semen Analysis: A Critical Review and SWOT Analysis, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC8706130/
Summary: Reference Values - LabCE.com, Laboratory Continuing Education, accessed May 21, 2025, https://www.labce.com/spg62845_summary_reference_values.aspx
Prognosis-based management of unexplained infertility—why not? - Oxford Academic, accessed May 21, 2025, https://academic.oup.com/hropen/article/2024/2/hoae015/7633735
ICSI vs. IVF: the correct choice - ESHRE, accessed May 21, 2025, https://www.eshre.eu/-/media/sitecore-files/SIGs/Embryology/Archive/Maribor/Reljic.pdf
Severe male factor in in vitro fertilization: definition, prevalence, and treatment. An update, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC8887096/
Contemporary Use of ICSI and Epigenetic Risks to Future Generations, accessed May 21, 2025, https://www.mdpi.com/2077-0383/11/8/2135
Superior Live Birth Rates, Reducing Sperm DNA Fragmentation (SDF), and Lowering Miscarriage Rates by Using Testicular Sperm Versus Ejaculates in Intracytoplasmic Sperm Injection (ICSI) Cycles from Couples with High SDF: A Systematic Review and Meta-Analysis - MDPI, accessed May 21, 2025, https://www.mdpi.com/2079-7737/14/2/130
Clinical Outcomes and Live Birth Rate Resulted From Microdissection Testicular Sperm Extraction With ICSI-IVF in Non-Obstructive Azoospermia: A Single-Center Cohort Study - Frontiers, accessed May 21, 2025, https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2022.893679/full
Intracytoplasmic sperm injection (ICSI) for non–male factor indications: a committee opinion (2020) | American Society for Reproductive Medicine, accessed May 21, 2025, https://www.asrm.org/practice-guidance/practice-committee-documents/intracytoplasmic-sperm-injection-icsi-for-nonmale-factor-indications-a-committee-opinion-2020/
www.britishfertilitysociety.org.uk, accessed May 21, 2025, https://www.britishfertilitysociety.org.uk/wp-content/uploads/2023/10/the-use-of-ICSI-in-ART.pdf
Opportunities and Limits of Conventional IVF versus ICSI: It Is Time to Come off the Fence, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9572455/
Quality statement 7: Intracytoplasmic sperm injection | Fertility problems - NICE, accessed May 21, 2025, https://www.nice.org.uk/guidance/qs73/chapter/quality-statement-7-intracytoplasmic-sperm-injection
Intracytoplasmic sperm injection | Information for the public | Fertility ..., accessed May 21, 2025, https://www.nice.org.uk/guidance/cg156/ifp/chapter/intracytoplasmic-sperm-injection
IVF-ICSI Split Insemination Reveals those Cases of Unexplained Infertility Benefitting from ICSI Even when the DNA Fragmentation Index is Reduced to 15% or Even 5% | SciTechnol, accessed May 21, 2025, https://www.scitechnol.com/peer-review/ivficsi-split-insemination-reveals-those-cases-of-unexplained-infertilitybenefitting-from-icsi-even-when-the-dna-fragmentation-ind-bV9X.php?article_id=4838
Case Number: 202201-144945 - Department of Financial Services, accessed May 21, 2025, https://www.dfs.ny.gov/public-appeals/case-number-202201-144945
Impact of intracytoplasmic sperm injection in women with ... - Frontiers, accessed May 21, 2025, https://www.frontiersin.org/journals/reproductive-health/articles/10.3389/frph.2022.1029381/full
ICSI Does Not Improve Live Birth Rates but Yields Higher Cancellation Rates Than Conventional IVF in Unexplained Infertility - Frontiers, accessed May 21, 2025, https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2020.614118/full
The role of ICSI vs. conventional IVF for patients with advanced maternal age—a randomized controlled trial - PMC, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC7822989/
Intracytoplasmic sperm injection compared with in vitro fertilisation in patients with non-male factor infertility with low oocyte retrieval: a single-centre, retrospective cohort study, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11575241/
Outcomes IVF vs ICSI in patients aged younger than 35 years. - ResearchGate, accessed May 21, 2025, https://www.researchgate.net/figure/Outcomes-IVF-vs-ICSI-in-patients-aged-younger-than-35-years_tbl1_255174724
Can Comprehensive Chromosome Screening Technology Improve IVF/ICSI Outcomes? A Meta-Analysis | PLOS One, accessed May 21, 2025, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0140779
Comparison of pregnancy rates for poor responders using IVF with mild ovarian stimulation versus conventional IVF: a guideline (2018) | American Society for Reproductive Medicine | ASRM, accessed May 21, 2025, https://www.asrm.org/practice-guidance/practice-committee-documents/comparison-of-pregnancy-rates-for-poor-responders-using-ivf-with-mild-ovarian-stimulation-versus-conventional-ivf-a-guideline-2018/
Reproductive Outcomes of Conventional In Vitro Fertilization and ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11090916/
Is ICSI More Effective Than IVF? Key Differences Explained - Inito Blogs, accessed May 21, 2025, https://blog.inito.com/ivf-vs-icsi/
Feasibility of preimplantation genetic testing for ... - Frontiers, accessed May 21, 2025, https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2024.1441014/full
(PDF) Pregnancy Outcomes, Miscarriage and Live Birth Rates ..., accessed May 21, 2025, https://www.researchgate.net/publication/377225655_Pregnancy_Outcomes_Miscarriage_and_Live_Birth_Rates_Following_the_Transfer_of_Thawed_Vitrified_Embryos_Derived_from_IVF_vs_ICSI_A_Retrospective_Analysis
Conventional IVF performs similarly in women with and without endometriosis - PMC, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10033814/
Intracytoplasmic Sperm Injection May Not Improve ... - Frontiers, accessed May 21, 2025, https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2022.877471/full
Intracytoplasmic Sperm Injection May Not Improve Clinical Outcomes Despite Its Positive Effect on Embryo Results: A Retrospective Analysis of 1130 Half-ICSI Treatments - Frontiers, accessed May 21, 2025, https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2022.877471/pdf
Conventional IVF versus ICSI in sibling oocytes from couples with endometriosis and normozoospermic semen - PMC, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3585678/
ICSI does not increase the cumulative live birth rate in non-male factor infertility - Oxford Academic, accessed May 21, 2025, https://academic.oup.com/humrep/article/33/7/1322/5036092
Live birth rates using conventional in vitro fertilization compared to intracytoplasmic sperm injection in Bologna poor responders with a single oocyte retrieved - PubMed Central, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC4429441/
Differences in fertilization, blastocyst, and ploidy rates in ..., accessed May 21, 2025, https://txfertility.com/research-studies/differences-in-fertilization-blastocyst-and-ploidy-rates-in-intracytoplasmic-sperm-injection-icsi-versus-conventional-insemination-for-patients-undergoing-in-vitro-fertilization-ivf-2/
effectiveness of ICSI versus conventional IVF in couples with non-male factor infertility: study protocol for a randomised controlled trial - Oxford Academic, accessed May 21, 2025, https://academic.oup.com/hropen/article/2019/2/hoz006/5420995
The effect of ICSI in infertility couples with non-male factor: a ..., accessed May 21, 2025, https://www.researchgate.net/publication/346312326_The_effect_of_ICSI_in_infertility_couples_with_non-male_factor_a_systematic_review_and_meta-analysis
Best practices of ASRM and ESHRE: a journey through reproductive medicine - Oxford Academic, accessed May 21, 2025, https://academic.oup.com/humrep/article/27/12/3365/653252
Use of ICSI in IVF cycles in women with tubal ligation does not improve pregnancy or live birth rates - PubMed Central, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC6457106/
The longer-term effects of IVF on offspring from childhood to ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9773093/
Best practices of ASRM and ESHRE: a journey through reproductive medicine, accessed May 21, 2025, https://www.asrm.org/practice-guidance/practice-committee-documents/best-practices-of-asrm-and-eshre-a-journey-through-reproductive-medicine-2012/
ufhealth.org, accessed May 21, 2025, https://ufhealth.org/sites/default/files/media/Repro-Subsite/ART-Consent-Form.pdf
Long-term health implications for children conceived by IVF/ICSI - ResearchGate, accessed May 21, 2025, https://www.researchgate.net/publication/24243042_Long-term_health_implications_for_children_conceived_by_IVFICSI
Assessing the Relationship Between Traditional In Vitro Fertilization and Birth Defects: A Systematic Review and Meta-Analysis - Journal of IVF-Worldwide, accessed May 21, 2025, https://jivfww.scholasticahq.com/article/91039-assessing-the-relationship-between-traditional-in-vitro-fertilization-and-birth-defects-a-systematic-review-and-meta-analysis"
(PDF) Birth defects in children conceived by ICSI compared with ..., accessed May 21, 2025, https://www.researchgate.net/publication/8165101_Birth_defects_in_children_conceived_by_ICSI_compared_with_children_conceived_by_other_IVF-methods_a_meta-analysis
School-age outcomes among IVF and ICSI-conceived children: a ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11963277/
The longer-term effects of IVF on offspring from childhood to ..., accessed May 21, 2025, https://www.frontiersin.org/journals/reproductive-health/articles/10.3389/frph.2022.1045762/full
The cost effectiveness of intracyctoplasmic sperm injection (ICSI) - PMC, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3454996/
The cost effectiveness of intracyctoplasmic sperm injection (ICSI) - ResearchGate, accessed May 21, 2025, https://www.researchgate.net/publication/5839231_The_cost_effectiveness_of_intracyctoplasmic_sperm_injection_ICSI
Economic evaluations of assisted reproductive technologies in high ..., accessed May 21, 2025, https://academic.oup.com/humrep/article/39/5/981/7618943
Applying a simplified economic evaluation approach to evaluate infertility treatments in clinical practice - PMC, accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10905501/
The impact of introducing patient co-payments in Germany on the use of IVF and ICSI: A price-elasticity of demand assessment - ResearchGate, accessed May 21, 2025, https://www.researchgate.net/publication/26688775_The_impact_of_introducing_patient_co-payments_in_Germany_on_the_use_of_IVF_and_ICSI_A_price-elasticity_of_demand_assessment
The economic impact of assisted reproductive technology: a review of selected developed countries | ICMART, accessed May 21, 2025, https://www.icmartivf.org/wp-content/uploads/7.-The-economic-impact-of-ART-a-review-of-selected-developed-countries.-.pdf
Talking about possible IVF/ICSI failure and need for multiple cycles in treatment planning: qualitative investigation of multi-cycle planning and its acceptability to patients and staff - Oxford Academic, accessed May 21, 2025, https://academic.oup.com/humrep/article/37/3/488/6510569
Artificial Intelligence in Reproductive Medicine – An Ethical ..., accessed May 21, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9833891/
Informed consent in assisted reproduction: an Ethics Committee opinion (2023) - ASRM, accessed May 21, 2025, https://www.asrm.org/practice-guidance/ethics-opinions/informed-consent-in-assisted-reproduction-an-ethics-committee-opinion-2023/
. . .
CARE Fertility and Women’s Health is a leading fertility clinic, offering personalized care and advanced reproductive technology to help individuals and couples achieve their dream of parenthood. With state-of-the-art genetic testing, individualized treatment plans, and holistic support, we specialize in complex fertility cases and boast some of the highest success rates in Canada.
Stay Informed!
Follow us on social media for fertility tips, patient stories, and the latest advancements in fertility care. Facebook | Instagram | LinkedIn | X | TikTok | YouTube