By CARE Fertility & Women’s Health
May 2025
Disclaimer: Please note that this medical review is intended for informational purposes only and should not be considered as medical advice. It has been prepared with the assistance of artificial intelligence and has not undergone peer review by medical professionals. Consult with a qualified healthcare provider for personalized medical guidance and treatment. The information provided herein is not a substitute for professional medical advice.
I. Introduction
The Journey to Conception: Understanding Your Options
The path to parenthood is a profound human experience, yet the journey to conception can vary significantly among individuals and couples. For many, pregnancy occurs readily, while for others, it may involve challenges and require medical assistance. This guide aims to provide a comprehensive overview of natural fertility and the landscape of fertility treatments, offering evidence-based information to support informed decision-making. Understanding the probabilities of conception, the factors that influence them, and the available interventions is a crucial first step for anyone embarking on or navigating this journey.
The Critical Role of Age and Other Factors in Fertility
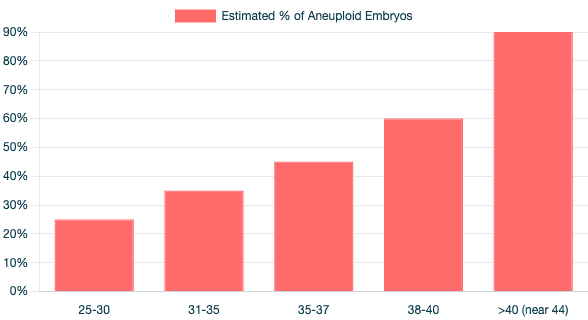
Chart: Embryo Aneuploidy by Maternal Age
Among the myriad factors influencing the ability to conceive, female age stands out as the most significant non-modifiable determinant¹. While a woman's peak reproductive years are typically in her late teens and twenties, fertility begins a natural decline from the early thirties, with a more pronounced decrease after the age of 35¹. This age-related decline affects not only the chances of natural conception but also the success rates of fertility treatments when using a woman's own eggs¹. Beyond female age, male factors, lifestyle choices, and underlying medical conditions in both partners also play substantial roles in the overall fertility equation.
It has been observed that societal trends towards delaying childbearing for educational or career pursuits mean that many individuals may only begin to focus on conception later in life.⁴ This delay can inadvertently lead to encountering age-related fertility challenges. The natural decline in fertility, particularly after 35, coupled with diminishing success rates of treatments like In Vitro Fertilization (IVF) using own eggs at older ages¹, highlights a potential "fertility awareness gap." A lack of early understanding about these biological timelines can result in individuals facing reduced natural fertility and potentially lower treatment success rates by the time they are ready to start a family. This situation underscores a broader need for public health education on fertility, empowering individuals to make timely and informed family planning decisions.
A Note on Interpreting Statistics: Population Averages vs. Individual Prognosis
The statistics presented throughout this guide are derived from large population studies and represent average probabilities. It is essential to recognize that these figures may not directly reflect an individual's or a couple's specific chances of achieving pregnancy¹. Personal fertility status is unique and influenced by a complex interplay of factors. Therefore, while this information serves as a valuable reference, personalized medical advice and assessment from healthcare professionals are indispensable for understanding individual prognosis and treatment options¹.
II. Natural Conception: Chances and Influencing Factors
A. Age-Specific Probabilities of Natural Pregnancy
The likelihood of conceiving naturally is intrinsically linked to female age. For women in their mid-twenties, the monthly chance of natural pregnancy is approximately 25%. This probability begins to decrease thereafter; for women over 30, the chance drops to around 20% per month, and by age 40, it is estimated to be less than 5% per month¹.
When considering the cumulative probability over a longer timeframe, such as one year of trying to conceive, the chances are higher, though still significantly impacted by age. Studies indicate the following 1-year cumulative probabilities of achieving a pregnancy (these figures generally refer to clinical pregnancy, as live birth rates can be slightly lower due to pregnancy loss):
Ages 20-24: Approximately 86%
Ages 25-29: Approximately 78%
Ages 30-34: Approximately 63%
Ages 35-39: Approximately 52%²
These figures underscore the progressive decline in natural fecundity with advancing age.
Table 1: Monthly and 1-Year Natural Conception (Clinical Pregnancy) Rates by Female Age
Age Group | Monthly Chance of Natural Conception (Clinical Pregnancy) | 1-Year Cumulative Chance of Natural Conception (Clinical Pregnancy) | Source (Monthly) | Source (Annual) |
20-24 | ~25% | 86% | 1 | 2 |
25-29 | ~25% | 78% | 1 | 2 |
30-34 | ~20% | 63% | 1 | 2 |
35-39 | <15% (e.g., 10-15%) | 52% | 1 | 2 |
40+ | <5% (e.g., 1-5%) | Data not specified, but significantly lower | 1 | - |
Note: "Chance of getting pregnant" is generally interpreted as clinical pregnancy unless live birth is specified.
B. Key Determinants of Natural Fertility
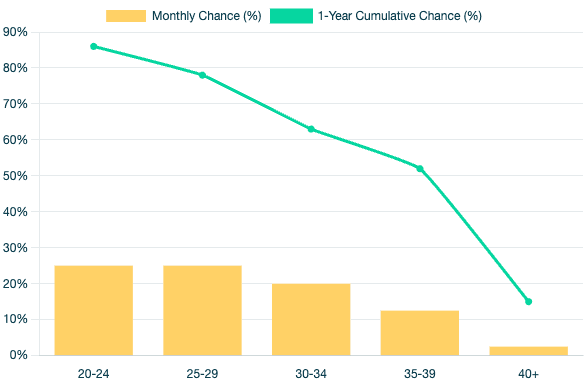
Chart: Natural Conception Rates by Age
Female Factors:
Ovarian Reserve (Egg Quantity and Quality): A woman is born with all the eggs she will ever possess, typically around one million at birth. This number diminishes to about half by puberty, and thereafter, up to 1,000 eggs are lost each month, with only one typically maturing and ovulating¹. This decline in egg quantity is measured by indicators like Anti-Müllerian Hormone (AMH), which also decreases with age (e.g., average AMH around 3.5 ng/ml at age 30, falling to 1.3 ng/ml at age 40, and 0.07 ng/ml after age 43)¹. Crucially, egg quality, primarily referring to chromosomal normality (euploidy), also deteriorates significantly with age¹.
Chromosomal Normality of Eggs (Aneuploidy): The proportion of eggs with chromosomal abnormalities (aneuploidy) increases substantially as a woman ages. For instance, the percentage of genetically abnormal embryos is estimated at 25% for women aged 25-30, rising to 35% for ages 31-35, 45% for ages 35-37, and 60% for ages 38-40¹. Other data suggest aneuploidy rates in eggs are around 20% at age 29, 35% at age 35, nearly 60% at age 40, and approaching 90% by age 44.2 This increase in aneuploidy directly correlates with a higher risk of genetically abnormal pregnancies, leading to implantation failure, miscarriage, or conditions like Down syndrome. The risk of a genetically abnormal pregnancy is about 1 in 475 at age 25, increasing to 1 in 178 at age 35, 1 in 62 at age 40, and 1 in 18 by age 45¹.
Male Factors:
Paternal Age: While often less emphasized than maternal age, paternal age also impacts fertility. Semen parameters can begin to decline as early as age 35.5 Men over 40 may experience a 30% lower likelihood of achieving conception with their partner within a 12-month period compared to men younger than 30.8 Furthermore, increasing paternal age, especially beyond 40-42, can reduce live birth rates even in IVF treatments, demonstrating an independent effect.⁵
Sperm Quality: Healthy sperm are essential for natural conception. Key parameters include count (concentration), motility (ability to swim), morphology (shape), and DNA integrity. Deficiencies in any of these areas can impair fertilization.⁵
Lifestyle and Environmental Factors (for both partners):
A range of modifiable lifestyle choices and environmental exposures can significantly influence both male and female fertility.
Diet & Nutrition: A diet rich in antioxidants, certain micronutrients (like folate and lycopene), fruits, and vegetables, and lower in protein and fats, has been correlated with improved semen quality in men. For women, replacing animal protein with vegetable protein and choosing monounsaturated fats over trans fats may be beneficial for ovulatory fertility.⁵
Weight (BMI): Both extremes of body weight can be detrimental. In men, obesity (BMI >30) is linked to reduced semen quality, increased sperm DNA damage, and erectile dysfunction.⁵ In women, obesity can lead to a longer time to pregnancy and a higher risk of miscarriage, while being underweight (BMI <17-18.5) is associated with ovarian dysfunction and infertility.⁵
Exercise: Moderate, regular exercise can be beneficial for male sperm parameters and can aid fertility in obese women when combined with weight loss. However, excessive or very high-intensity exercise can negatively alter energy balance and hormonal function, potentially impairing fertility in both sexes.⁵
Smoking, Alcohol, Caffeine, Illicit Drugs:
Smoking: Adversely affects male fertility by reducing sperm count, motility, and morphology, and increasing DNA damage. In women, smoking is linked to infertility, reduced ovarian reserve, and hormonal disruptions.⁵
Alcohol: Chronic heavy alcohol use can cause testicular atrophy and decrease sperm parameters in men. In women, significant alcohol consumption can increase time to pregnancy, decrease conception probability, and raise the risk of miscarriage.⁵
Caffeine: High caffeine intake (e.g., >500 mg/day) has been associated with increased time to pregnancy and a higher risk of miscarriage.⁵
Illicit Drugs: Substances like marijuana, cocaine, and opiates can negatively impact reproductive function in both men and women, affecting hormone levels, sperm production, ovulation, and fetal development.⁵
Psychological Stress: Significant life stress can negatively impact sperm parameters in men and hormonal regulation in women, potentially affecting conception rates and pregnancy outcomes.⁵
Occupational/Environmental Exposures: Exposure to air pollution, heavy metals (like lead and mercury), pesticides, and certain industrial chemicals can have substantial negative effects on fertility. These substances can disrupt hormonal balance, damage gametes, and lead to adverse reproductive outcomes such as miscarriage or fetal malformations.⁵ The impact of these environmental factors can be insidious, as individuals may be unaware of their exposure through daily life or specific occupations. This highlights a potential under-recognized contribution to infertility that is often harder to identify and mitigate compared to more direct lifestyle choices.
The interplay of multiple lifestyle factors is also noteworthy. While individual elements like smoking or high BMI have known negative impacts, their combined effect can be more substantial. For example, one study indicated that couples exhibiting four adverse lifestyle factors had a 38% conception rate over 12 months, compared to 83% for those with no such factors.⁶ This suggests an additive, or possibly synergistic, negative impact. Therefore, a holistic approach to preconception health, addressing multiple areas simultaneously, may offer greater fertility benefits than focusing on a single factor. Even seemingly "mild" individual risk factors can collectively create a significant barrier to conception.
Intercourse Timing and Frequency:
Understanding the fertile window—typically the six days leading up to and including ovulation—and timing intercourse during this period is important for maximizing the chances of natural conception.
III. When to Seek Help: An Overview of Fertility Treatments
Common Reasons for Considering Fertility Assistance
Couples or individuals may consider seeking fertility assistance for a variety of reasons. These commonly include age-related decline in fertility, ovulatory disorders such as Polycystic Ovary Syndrome (PCOS), blockages in the fallopian tubes (tubal factor infertility), male factor infertility (issues with sperm count, motility, or morphology), endometriosis, or when no specific cause is identified after investigation (unexplained infertility).⁹ It is estimated that approximately 10% of women of reproductive age in the United States face challenges in becoming pregnant or carrying a pregnancy to term¹. Guidelines often suggest consultation after one year of trying to conceive for women under 35, or after six months for women 35 and older, or sooner if specific risk factors are present.
Brief Introduction to the Spectrum of Treatments
Fertility treatments range from simpler, less invasive interventions to more complex assisted reproductive technologies (ART). The approach is often tiered, starting with methods aimed at enhancing natural processes before moving to more advanced options if necessary. These treatments include lifestyle modifications, ovulation induction with timed intercourse, intrauterine insemination (IUI), and in vitro fertilization (IVF).
IV. Ovarian Stimulation with Timed Intercourse (OS-TI)
A. Understanding OS-TI: The Procedure
Ovarian Stimulation with Timed Intercourse (OS-TI) is a fertility treatment designed to increase the chances of natural conception by ensuring the development of one or more mature eggs and precisely timing sexual intercourse to coincide with ovulation¹. It is often considered a first-line, less invasive treatment option.
The typical steps involved in an OS-TI cycle are:
Initial Evaluation & Testing: Before starting treatment, both partners undergo standard fertility assessments. For the female partner, this includes blood tests to evaluate hormone levels (like FSH, LH, estradiol, AMH) and ovarian function, along with transvaginal ultrasounds to assess reproductive anatomy. For the male partner, a semen analysis is conducted to measure sperm count, motility, and morphology.¹⁴
Baseline Ultrasound: At the beginning of the menstrual cycle (or after inducing a period if cycles are irregular), a transvaginal ultrasound is performed to examine the ovaries for any large cysts that might interfere with treatment. If the ovaries appear normal, the cycle proceeds.¹⁴
Ovulation Stimulation with Medication: Medications are prescribed to stimulate the ovaries to produce mature eggs. These can be oral medications like clomiphene citrate (Clomid) or letrozole, usually taken for about five days, or injectable gonadotropins (FSH), typically administered for 8-12 days depending on ovarian response.¹⁴ The general principles of ovarian stimulation, such as pre-stimulation management and monitoring, are guided by established reproductive medicine practices.¹⁶
Monitoring Follicle Growth: The response to medication is closely monitored with transvaginal ultrasounds and sometimes blood tests (e.g., estradiol levels) every 2-5 days. This allows the physician to track the number and size of developing follicles and adjust medication dosages if necessary.¹⁴ The goal is often to achieve one to three mature follicles to balance pregnancy chances with the risk of multiple pregnancies.
Trigger Shot: When one or more follicles reach an optimal size (typically 18-20 mm), an injection of human chorionic gonadotropin (hCG) or a GnRH agonist is administered. This "trigger shot" mimics the natural LH surge and induces final egg maturation and ovulation, usually within 36-42 hours.¹⁴
Timed Intercourse: The couple is advised to have sexual intercourse daily or every other day for approximately three consecutive days, timed to coincide with the expected ovulation period following the trigger shot.¹⁴
Progesterone Monitoring/Support: About one week after ovulation, a blood test may be done to measure progesterone levels to confirm ovulation and ensure adequate support for the uterine lining. If progesterone levels are low, supplemental progesterone (oral or vaginal) may be prescribed.¹⁴
Pregnancy Testing: A pregnancy test (blood or urine) is typically performed about two weeks after ovulation.¹⁴
OS-TI is commonly indicated for women with irregular or absent ovulation (anovulation), certain hormonal abnormalities, unexplained infertility, or couples with mild male factor infertility where sperm parameters are only slightly suboptimal.¹⁴
B. Success Rates of OS-TI
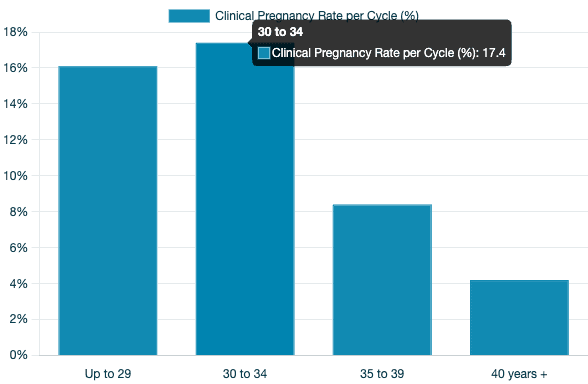
Chart: OS-TI Clinical Pregnancy Rates
Success rates for OS-TI are influenced by various factors, most notably female age. A study conducted in Brazil focusing on couples with unexplained subfertility undergoing OS-TI reported the following clinical pregnancy rates per cycle¹⁷:
Up to 29 years: 16.1%
30 to 34 years: 17.4%
35 to 39 years: 8.4%
40 years and older: 4.2%
In the same study, the overall patient-based clinical pregnancy rate was 18.55% per patient who started treatment, and the cycle-based clinical pregnancy rate was 13.14% per cycle initiated. Some patients achieved pregnancy more than once over the course of up to six attempts, leading to a cumulative clinical pregnancy rate of 21.4% within that cohort.¹⁷ Live birth rates are generally expected to be somewhat lower than clinical pregnancy rates due to the possibility of miscarriage.
Table 2: OS-TI Clinical Pregnancy Rates per Cycle by Female Age (Unexplained Subfertility)
Female Age Group | Clinical Pregnancy Rate per Cycle (OS-TI) | Source |
Up to 29 years | 16.1% | 17 |
30 to 34 years | 17.4% | 17 |
35 to 39 years | 8.4% | 17 |
40 years + | 4.2% | 17 |
Source: Radaelli et al. 2022. Rates are clinical pregnancy rates.
C. Factors Influencing OS-TI Success
Female Age: This is a primary determinant. The Radaelli et al. study (2022) indicated that for each additional year in the woman's age, the likelihood of pregnancy decreased by approximately 6.45%.¹⁷
Sperm Parameters: The quality of the male partner's sperm is crucial. The same study found that cycles where the total motile sperm count (TMSC) was 5 million or greater had a 1.91 times higher chance of resulting in pregnancy compared to cycles with TMSC below 5 million.¹⁷
Ovarian Response and Reserve: A woman's ability to respond to stimulation medications, often reflected by markers like AMH, plays a role. The study noted that women who conceived had, on average, higher AMH levels [¹⁷ (Table 4)].
Underlying Cause of Infertility: While the cited study focused on unexplained subfertility, the effectiveness of OS-TI logically depends on whether the ovarian stimulation and timed intercourse address the specific root cause of infertility. For example, it is particularly effective for anovulatory infertility.
For couples with unexplained subfertility, OS-TI is often considered a first-line treatment due to its lower invasiveness and cost compared to more complex procedures like IVF.¹⁷ Its success rates, though modest and highly age-dependent, can also provide valuable prognostic information. If pregnancy occurs, it suggests that subtle ovulatory or timing issues may have been the primary barrier. Conversely, if several OS-TI cycles fail, particularly in younger women with good sperm parameters, it might indicate the presence of other underlying factors not effectively addressed by this method, such as issues with fertilization, implantation, or more significant egg quality decline. In such cases, these outcomes can help guide the decision to move towards more advanced treatments like IUI or IVF. Thus, OS-TI can function not only as a therapeutic intervention but also as a diagnostic step, refining the understanding of a couple's fertility challenges.
V. Intrauterine Insemination (IUI)
A. Understanding IUI: The Procedure
Intrauterine Insemination (IUI) is a fertility treatment that involves placing specially prepared (washed) sperm directly into a woman's uterus around the time of ovulation.⁹ The primary goal is to bypass the cervix, increasing the number of motile sperm that reach the fallopian tubes, thereby enhancing the probability of fertilization.
IUI can be performed in two main ways:
Natural Cycle IUI:
Process: This approach involves monitoring the woman's natural menstrual cycle using methods like ovulation predictor kits (which detect the LH surge) or transvaginal ultrasound to track follicle development. The IUI procedure is timed to coincide with natural ovulation. No ovarian stimulation medications are used.¹⁰
Indications: Natural cycle IUI is often considered for couples with infertility due to cervical factors (where cervical mucus may be hostile to sperm), or when the male partner has ejaculatory dysfunction, provided the female partner has regular ovulation and patent fallopian tubes.¹¹ Some research suggests it may be a preferable option for women over 37 years compared to stimulated IUI, although this is an area of ongoing discussion.¹¹
Ovarian Stimulation IUI (COH-IUI / OS-IUI):
Process: This method combines controlled ovarian hyperstimulation (COH), also known as ovarian stimulation (OS), with the IUI procedure. Similar to OS-TI, medications such as clomiphene citrate, letrozole, or injectable gonadotropins are used to encourage the development of one to three mature follicles.⁹ The cycle involves careful monitoring of follicle growth via ultrasound and sometimes blood tests, administration of a trigger shot (e.g., hCG) to induce ovulation, and then performing the IUI procedure at the optimal time.¹⁰
Indications: OS-IUI is commonly recommended for couples with unexplained infertility, mild to moderate male factor infertility (where sperm parameters are slightly reduced but still adequate for IUI after preparation), ovulation dysfunctions (like PCOS), and minimal or mild endometriosis.⁹
Sperm Preparation: Regardless of whether the cycle is natural or stimulated, the male partner provides a semen sample on the day of the IUI. This sample undergoes a laboratory process called "sperm washing" or preparation. This procedure separates the motile sperm from the seminal fluid, white blood cells, prostaglandins, and other debris, concentrating the healthiest sperm in a small volume for insemination.⁹
B. Success Rates of IUI
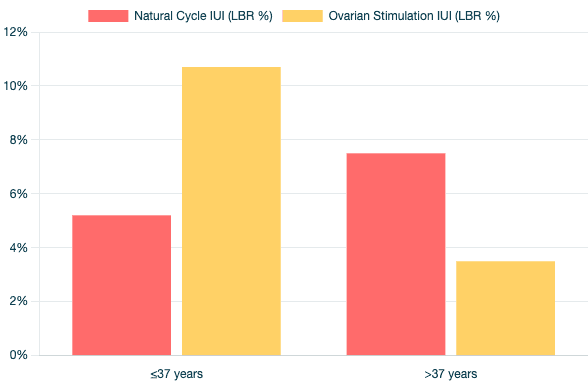
Chart: IUI Live Birth Rates
Success rates for IUI can vary widely depending on numerous factors, including the woman's age, the cause of infertility, whether ovarian stimulation is used, and sperm quality. Reported clinical pregnancy rates per cycle for OS-IUI generally range from 10% to 20% in selected patient populations, though some reviews cite ranges as wide as 5% to 70% under varying conditions.⁹ Live birth rates are typically a few percentage points lower than clinical pregnancy rates.
Natural Cycle IUI vs. Ovarian Stimulation IUI (Live Birth Rate per cycle for unexplained infertility, from Kalu et al.):
A retrospective study comparing natural cycle IUI with COH-IUI in women with unexplained infertility reported the following live birth rates per cycle¹⁸:
Natural Cycle IUI:
Women ≤37 years: 5.2%
Women >37 years: 7.5%
Ovarian Stimulation IUI (COH-IUI):
Women ≤37 years: 10.7%
Women >37 years: 3.5% (specifically, with clomiphene citrate stimulation, the live birth rate was 2.1% for women >37 years).
Age-Specific OS-IUI Success (Clinical Pregnancy per cycle, from various sources):
Women under 35 years: Approximately 15-20%.¹³
Women aged 35-40 years: Approximately 10%.¹³
Women over 40 years: Approximately 2-5%.¹³
European Data (ESHRE 2019 Report, Delivery Rate per cycle)²²:
IUI-H (using husband/partner's sperm): 8.7% overall delivery rate.
IUI-D (using donor sperm): 12.1% overall delivery rate. (It's important to note that donor sperm is often utilized by younger women, women without male partners, or same-sex female couples, which may contribute to the higher success rates observed compared to IUI-H).
Cumulative Success Rates:
Since per-cycle success rates for IUI are modest, multiple cycles are often recommended, typically up to three to six attempts, before considering more advanced treatments like IVF.⁹
For couples with unexplained infertility, one study reported a cumulative live birth rate of 26.5% after two to three OS-IUI cycles.²⁴
Another source suggests cumulative clinical pregnancy rates after three OS-IUI cycles using letrozole or clomiphene can range from 15-25%.²¹
Table 3: IUI Live Birth Rates per Cycle by Female Age: Natural vs. Stimulated Cycles (Unexplained Infertility)
Treatment Type | Female Age Group | Live Birth Rate per Cycle | Source |
Natural Cycle IUI | ≤37 years | 5.2% | 18 |
Natural Cycle IUI | >37 years | 7.5% | 18 |
OS-IUI (Stimulated) | ≤37 years | 10.7% | 18 |
OS-IUI (Stimulated) | >37 years | 3.5% | 18 |
Source: Kalu et al. (2007). Rates are live birth rates per cycle for unexplained infertility.
C. Factors Influencing IUI Success
The success of IUI is contingent upon several key factors:
Female Age: This is consistently one of the most critical factors. Success rates generally decline significantly after the age of 35-37 years.⁹
Male Age: While less impactful than female age, increasing paternal age (especially beyond 35-40 years) can also be a contributing factor to lower success rates.⁹
Type and Duration of Infertility: IUI is more likely to be successful if the duration of infertility is shorter (e.g., less than 4-5 years).⁹ The underlying cause (etiology) of infertility is also paramount. IUI shows better outcomes for cervical factor infertility or anovulation but is less effective for severe male factor infertility, significant tubal disease, or severe endometriosis.⁹
Sperm Parameters (Post-Wash): The quality of the sperm after laboratory preparation is a major predictor. A higher total motile sperm count (TMSC) post-wash is associated with better outcomes; many clinics consider a TMSC of >5-10 million motile sperm to be favorable.⁹ Sperm morphology (shape) and progressive motility are also important.⁹
Number of Mature Follicles (for OS-IUI): In stimulated cycles, the aim is often to develop 1 to 3 mature follicles. Some studies suggest higher pregnancy rates with two follicles compared to one, but this also increases the risk of multiple pregnancies (twins, triplets).⁹ Therefore, strict cancellation criteria are often applied if more than three or four dominant follicles develop to mitigate this risk.²³
Endometrial Thickness: A receptive uterine lining (endometrium) is necessary for implantation. An endometrial thickness of ≥7mm on the day of the trigger shot or IUI is generally considered favorable.⁹
Ovulation Induction Protocol (for OS-IUI): The choice of medication for ovarian stimulation can influence outcomes. Some studies suggest that gonadotropins (injectable hormones) may yield higher pregnancy rates compared to oral anti-estrogens like clomiphene citrate in certain patient populations, although this is not universally conclusive and depends on the specific patient profile.¹⁰
Timing of Insemination: Precise timing of the IUI procedure relative to ovulation (either natural or triggered) is crucial for success, as both sperm and egg have limited lifespans.¹⁰
Previous Pregnancy History: Generally, a prior live birth is a positive prognostic indicator. However, a history of recurrent pregnancy loss, in the absence of known chromosomal abnormalities in the parents or significant uterine malformations, may not significantly reduce the chances of live birth with IUI or frozen embryo transfer cycles after fertility treatment.²⁷
The effectiveness of IUI is highly dependent on careful patient selection. It is most successful for younger women (typically under 35-37 years) who have patent fallopian tubes, normal or easily correctable ovulation, adequate ovarian reserve, and are experiencing unexplained infertility, cervical factor infertility, or mild male factor infertility (with good post-wash sperm parameters), and a shorter duration of infertility.⁹ IUI does not bypass significant issues related to advanced maternal age (poor egg quality), severe sperm dysfunction, blocked fallopian tubes, or severe endometriosis. For individuals outside this "sweet spot," transitioning to IVF more promptly might be a more effective strategy.
An interesting consideration arises for women over 37. While ovarian stimulation generally boosts IUI success in younger women, some research indicates that natural cycle IUI might yield comparable or even slightly better live birth rates for women over 37 compared to stimulated cycles, particularly those using clomiphene.¹¹ One retrospective study reported a 7.5% live birth rate for natural cycle IUI versus 3.5% for stimulated IUI (and 2.1% for clomiphene-IUI) in this older age group.¹⁸ This could be because the ovarian stimulation drugs, especially anti-estrogens like clomiphene, might negatively affect endometrial receptivity or the quality of the already more fragile oocytes in older women. A natural cycle allows the body's own mechanisms to select a dominant follicle, potentially avoiding these adverse effects. While this finding warrants cautious interpretation and further research, it suggests that for women over 37 considering IUI, a nuanced discussion about the pros and cons of natural versus stimulated cycles is important.
VI. In Vitro Fertilization (IVF)
A. Understanding IVF: The Step-by-Step Process
In Vitro Fertilization (IVF) is an advanced assisted reproductive technology that involves combining eggs and sperm outside the body in a laboratory setting. If fertilization occurs, the resulting embryo(s) are cultured for several days before one or more are transferred into the woman's uterus with the hope of implantation and pregnancy.²⁹ IVF is used to treat a wide range of infertility causes, including tubal factor, male factor, endometriosis, ovulatory disorders, age-related infertility, and unexplained infertility.²⁹
The IVF process generally involves the following key steps²⁹:
Pre-stimulation Treatment/Ovarian Suppression: In many protocols, treatment begins in the cycle preceding ovarian stimulation. This may involve oral contraceptive pills to help with cycle timing and prevent ovarian cysts. Medications like GnRH agonists (e.g., Lupron) or GnRH antagonists (e.g., Ganirelix, Cetrotide) are used to suppress the woman's natural hormones, preventing premature ovulation and allowing the physician to control the cycle.³⁰ A baseline pelvic ultrasound and blood tests are performed to ensure the ovaries are quiescent before stimulation begins.³⁰
Ovarian Stimulation (Controlled Ovarian Hyperstimulation): Injectable gonadotropin medications, containing follicle-stimulating hormone (FSH) and sometimes luteinizing hormone (LH), are administered daily for approximately 8 to 14 days. These hormones stimulate the ovaries to produce multiple mature eggs, rather than the single egg that typically develops in a natural cycle.²⁹
Monitoring Follicle Development: The response to ovarian stimulation is closely monitored through frequent transvaginal ultrasound examinations (to measure the number and size of developing follicles) and blood tests (to measure hormone levels, particularly estradiol).²⁹ Medication dosages may be adjusted based on these results.
Trigger Shot for Final Egg Maturation: When the follicles reach an appropriate size and maturity (typically when lead follicles are 18-22mm), an injection of human chorionic gonadotropin (hCG) or a GnRH agonist is given. This "trigger shot" mimics the natural LH surge and induces the final maturation of the eggs, preparing them for fertilization. Egg retrieval is scheduled approximately 34 to 36 hours after this injection, before ovulation would naturally occur.²⁹
Egg Retrieval (Oocyte Aspiration): This is a minor surgical procedure, usually performed under intravenous sedation or anesthesia in a procedure room or outpatient center. Using transvaginal ultrasound guidance, a thin needle is passed through the vaginal wall and into each ovarian follicle. The fluid from each follicle, containing the egg, is gently aspirated.²⁹ The procedure typically takes less than 30 minutes.
Sperm Preparation: On the day of egg retrieval, the male partner provides a semen sample (or a previously cryopreserved sample is thawed). The sperm is then processed in the laboratory to select the healthiest, most motile sperm.²⁹
Fertilization: The retrieved eggs are combined with the prepared sperm in the laboratory. This can be done in two ways:
Conventional Insemination: A concentrated number of motile sperm (e.g., 50,000 to 100,000) are placed in a culture dish with each egg and incubated overnight, allowing fertilization to occur naturally.²⁹
Intracytoplasmic Sperm Injection (ICSI): If there are concerns about sperm quality (low count, poor motility or morphology) or a history of failed fertilization with conventional IVF, ICSI is performed. In this technique, a single sperm is selected and injected directly into the cytoplasm of each mature egg using a specialized micromanipulation microscope.²⁹
Embryo Culture: Eggs are checked for fertilization the day after retrieval (typically 16-18 hours post-insemination/ICSI). Successfully fertilized eggs, now called embryos (or zygotes at the earliest stage), are placed in a specialized culture medium and grown in a controlled laboratory incubator for 3 to 7 days. Embryos develop through various stages, from cleavage stage (2-8 cells by day 2-3) to the blastocyst stage (a more advanced embryo with many cells forming a fluid-filled cavity, typically by day 5-7).²⁹
Embryo Transfer: One or more embryos are selected for transfer into the woman's uterus. This procedure is usually performed 3 to 5 days after egg retrieval (at cleavage or blastocyst stage). It is typically painless and does not require anesthesia. A thin, flexible catheter containing the embryo(s) in a small amount of culture medium is gently passed through the cervix and into the uterine cavity, where the embryo(s) are deposited.²⁹ The number of embryos transferred is carefully considered based on the woman's age, embryo quality, and previous IVF history, aiming to maximize the chance of pregnancy while minimizing the risk of high-order multiple pregnancies (twins, triplets, etc.).³²
Luteal Phase Support: Progesterone medication (and sometimes estrogen) is prescribed starting around the time of egg retrieval or embryo transfer to support the uterine lining (endometrium) and encourage embryo implantation. This support is typically continued until a pregnancy test is done, and if positive, often through the first 8-12 weeks of pregnancy [¹⁶ (general principle)].
Pregnancy Test: A blood test to measure hCG levels is usually performed 9 to 14 days after the embryo transfer to determine if pregnancy has occurred.
Any good-quality embryos that are not transferred can often be cryopreserved (frozen) for future use, a process known as vitrification.²⁹ This allows for subsequent frozen embryo transfer (FET) cycles without needing to repeat ovarian stimulation and egg retrieval.
B. Success Rates of IVF (Using Own Eggs)

Charts: IVF Success Rates
IVF success rates are most significantly influenced by the age of the woman providing the eggs, as this directly correlates with egg quality. Rates are typically reported as live births per cycle started, per egg retrieval, or per embryo transfer.
United States Data (SART 2022 National Summary) - Live Births Using Patient's Own Eggs³:
Live Births Per Intended Egg Retrieval (including all fresh and frozen embryo transfers within 1 year of retrieval): This metric provides a comprehensive view of the chance of having a baby from one ovarian stimulation cycle.
Women < 35 years: 53.5%
Women 35-37 years: 39.8%
Women 38-40 years: 25.6%
Women 41-42 years: 13.0%
Women > 42 years: 4.5%
Live Births From the First Embryo Transfer (fresh or frozen) after an egg retrieval cycle:
As a percentage of cycle starts for that first transfer attempt:
Women < 35 years: 39.4%
Women 35-37 years: 30.6%
Women 38-40 years: 20.9%
Women 41-42 years: 11.2%
Women > 42 years: 3.9%
As a percentage of embryo transfers performed for that first transfer:
Women < 35 years: 52.7%
Women 35-37 years: 40.0%
Women 38-40 years: 28.4%
Women 41-42 years: 16.8%
Women > 42 years: 6.6%
United Kingdom Data (HFEA 2022 Preliminary Report) - Live Birth Rate per Fresh Embryo Transferred, Using Patient's Own Eggs³³:
Women 18-34 years: 35%
Women 35-37 years: 26%
Women 38-39 years: 18%
Women 40-42 years: 10%
Women 43-44 years: 5%
The average IVF live birth rate using frozen embryo transfers (own eggs) was approximately 30% in 2022. Success with frozen embryos is largely dependent on the age of the woman at the time the embryos were created (frozen), rather than her age at the time of transfer.³³
European Data (ESHRE 2019 Report) - Using Patient's Own Eggs²²:
Clinical Pregnancy Rate per fresh IVF/ICSI embryo transfer: 34.6% overall.
Clinical Pregnancy Rate per thawing for frozen embryo transfer (own eggs): 35.1% overall. (Note: These are clinical pregnancy rates, not live birth rates, which are typically lower).
Cumulative Live Birth Rates (CLBR) over Multiple IVF Cycles:
Persistence through multiple IVF cycles can increase the overall chance of success. A UK-based study (1999-2007 cohort) found that after three complete IVF cycles (one fresh cycle plus any resulting frozen embryo transfers from that stimulation), the optimal cumulative live birth rate was 57.1%. After eight complete cycles, the optimal CLBR reached 82.4%.³⁵
A study from a Middle Eastern referral center reported an overall CLBR of 67.9% after 6 fresh IVF cycles. For women younger than 35 years, the CLBR reached 69.9% after 6 cycles. However, for women older than 40, the live birth rate for the first cycle was significantly lower at 3.1%, with CLBRs plateauing around 21.9% after 4 cycles.³⁶
The stark difference in success when using donor eggs further highlights the impact of oocyte age. IVF with young donor eggs (from donors typically in their 20s) yields live birth rates around 50-55% per transfer, and these rates remain relatively stable regardless of the recipient's age.¹ For example, 2021 CDC data indicated a 53.9% live birth rate for fresh donor eggs and 45.8% for frozen donor eggs.³⁷ This underscores that oocyte quality is a primary driver of IVF success.
Table 4: IVF Live Birth Rates (Own Eggs) by Female Age (SART 2022 Data, USA)
Female Age Group | Live Births Per Intended Egg Retrieval (All Embryo Transfers within 1 year of retrieval) | Live Births From First Embryo Transfer (as % of cycle starts for that transfer) | Live Births From First Embryo Transfer (as % of transfers performed) | Source |
< 35 years | 53.5% | 39.4% | 52.7% | 3 |
35-37 years | 39.8% | 30.6% | 40.0% | 3 |
38-40 years | 25.6% | 20.9% | 28.4% | 3 |
41-42 years | 13.0% | 11.2% | 16.8% | 3 |
> 42 years | 4.5% | 3.9% | 6.6% | 3 |
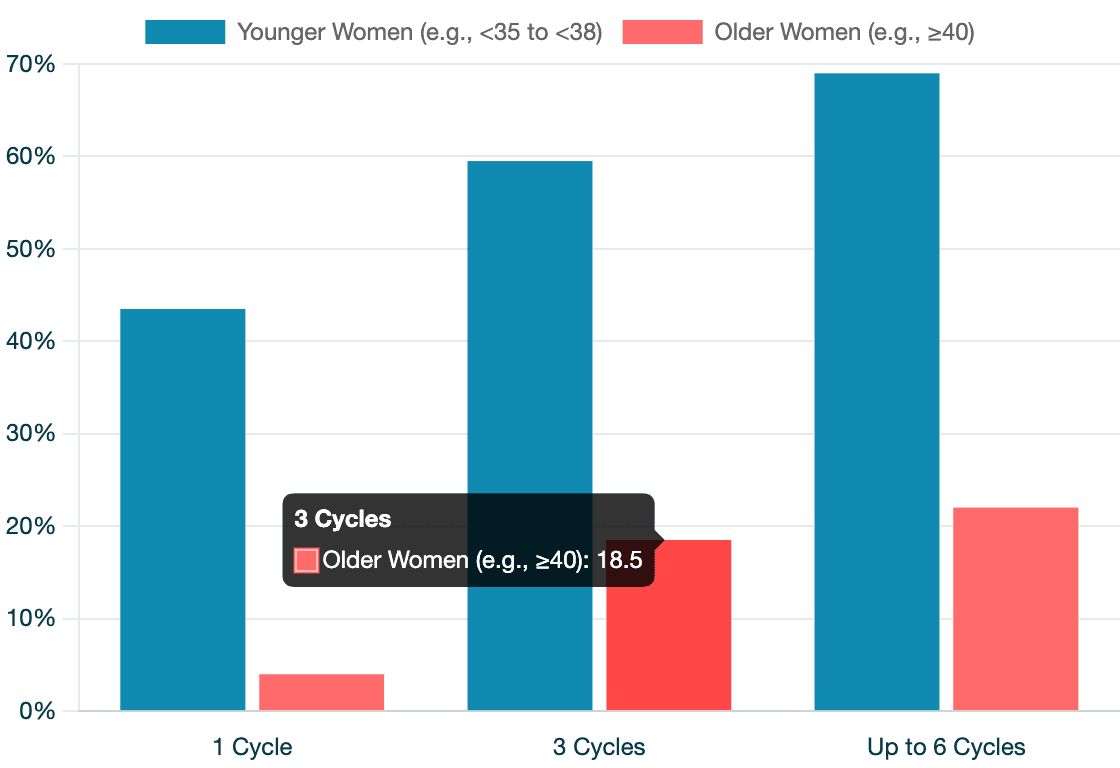
Table 5: Illustrative Cumulative IVF Live Birth Rates (Own Eggs) over Multiple Cycles
Number of Complete/Fresh Cycles | Illustrative Cumulative Live Birth Rate (Younger Women, e.g., <35 to <38) | Illustrative Cumulative Live Birth Rate (Older Women, e.g., ≥40) | Notes / Primary Sources |
1 Cycle | 33-54% | 3-5% | Range reflects different studies/metrics (per fresh cycle vs. per retrieval with all FETs).³ |
3 Cycles | 57-62% | ~15-22% (may plateau earlier) | Optimal CLBR after 3 complete cycles (UK study, 1999-2007) was 57.1%. ME study <35yrs: 61.7% after 3 fresh. ME study >40yrs: 21.9% after 4 fresh.³⁵ |
Up to 6 Cycles | 68-70% | ~22% (plateaued earlier) | ME study overall: 67.9% after 6 fresh. ME study <35yrs: 69.9% after 6 fresh.³⁶ |
Up to 8 Cycles | ~82% | Data limited / plateaued | Optimal CLBR after 8 complete cycles (UK study, 1999-2007) was 82.4%.³⁵ |
Note: "Complete cycle" in UK study includes fresh + subsequent frozen transfers from that retrieval. ME study data is for fresh cycles. These are illustrative ranges based on available data; individual prognosis varies.
C. Factors Influencing IVF Success
Numerous factors contribute to the outcome of an IVF cycle:
Female Age: This is the single most important predictor of success when using a woman's own eggs. Advancing maternal age is associated with a decline in both the quantity and, more critically, the quality (chromosomal normality or euploidy) of eggs.¹
Ovarian Reserve: Markers such as Anti-Müllerian Hormone (AMH) levels and Antral Follicle Count (AFC) can predict how well the ovaries will respond to stimulation (i.e., the number of eggs retrieved) but are less direct predictors of egg quality.⁴⁰ Women with low ovarian reserve tend to have lower cumulative live birth rates.³⁶
Embryo Quality: The viability of the embryo is paramount. Embryos are typically assessed morphologically (based on appearance and development rate). Preimplantation Genetic Testing for Aneuploidy (PGT-A) is an increasingly used technology that screens embryos for chromosomal abnormalities before transfer. The aim is to select euploid (chromosomally normal) embryos, which may improve implantation rates and reduce miscarriage rates, particularly for older women or those with recurrent implantation failure, though its routine use across all patient groups is still debated.⁴¹ Transferring chromosomally normal embryos (often identified via Comprehensive Chromosomal Screening - CCS, a form of PGT-A) results in high live birth rates (e.g., 62-73% per transfer depending on age group) and low miscarriage rates (around 4-6%), with success being less dependent on the maternal age at the time of transfer, provided a euploid embryo is available.⁴³ This reinforces that oocyte/embryo chromosomal status is a key determinant.
Number of Embryos Transferred: Historically, transferring multiple embryos was common to increase pregnancy chances, but this led to high rates of multiple pregnancies (twins, triplets), which carry risks for both mother and babies. There is a strong global trend towards elective Single Embryo Transfer (eSET), especially with good quality blastocysts, to reduce these risks.³
Cause of Infertility:
Polycystic Ovary Syndrome (PCOS): Women with PCOS often retrieve many eggs but may have concerns regarding oocyte quality or endometrial receptivity. They are also at higher risk of Ovarian Hyperstimulation Syndrome (OHSS). Pregnancies in women with PCOS may also have increased risks of complications.³⁹
Endometriosis: This condition can negatively impact fertility by affecting oocyte and embryo quality, impairing fallopian tube function, and altering the uterine environment due to inflammation. Severe endometriosis can cause pelvic adhesions and distort anatomy.¹¹
Male Factor Infertility: ICSI is highly effective in overcoming most male factor issues by directly injecting sperm into the egg. However, very severe sperm DNA fragmentation can still negatively influence outcomes.²⁹
Unexplained Infertility: IVF can be successful by bypassing potential undiagnosed problems with natural fertilization or early embryo development.
Lifestyle Factors: As with natural fertility, factors like smoking, obesity, and poor diet can negatively affect IVF outcomes, potentially impacting egg/sperm quality, ovarian response, or implantation.⁵
Previous Pregnancy History: A history of a previous live birth is generally a favorable prognostic factor. For women with a history of recurrent pregnancy loss (RPL), if obvious parental chromosomal issues or uterine malformations are excluded, their live birth rates in subsequent frozen embryo transfer cycles may not be significantly different from those without RPL.²⁷
Clinic-Specific Practices and Laboratory Quality: Variations in ovarian stimulation protocols, laboratory expertise in embryology (culture conditions, cryopreservation techniques), and overall quality control measures can influence IVF success rates between different clinics.⁴⁰
Number of Oocytes Retrieved and Embryos Available: Generally, retrieving a higher number of oocytes provides a better chance of obtaining more high-quality embryos, which increases the likelihood of having at least one good embryo for transfer and potentially others for cryopreservation.³⁹ However, an excessively high number of oocytes can sometimes be associated with a risk of OHSS or, in some cases, a slight compromise in average oocyte quality.
The field of IVF has seen a significant shift towards utilizing Frozen Embryo Transfers (FET). Many clinics now opt for "freeze-all" cycles, where all viable embryos from a stimulation cycle are cryopreserved, and transfer occurs in a subsequent, more natural or programmed endometrial cycle.³³ This approach is driven by several factors: the ovarian stimulation process creates a hormonal environment that may not be optimal for immediate embryo implantation; FET allows the endometrium to recover and be prepared under more physiological conditions; advances in vitrification (fast freezing) have dramatically improved embryo survival and viability post-thaw; and procedures like PGT-A necessitate freezing embryos while genetic testing is performed.²² Consequently, success rates with FET are often comparable to, or in some cases even better than, fresh transfers. This trend means that evaluating success "per egg retrieval" (encompassing all transfers from that retrieval) offers a more complete picture of a cycle's potential.
The data from donor egg IVF and PGT-A consistently underscore that oocyte quality is paramount. The high and stable success rates of donor egg IVF, irrespective of the recipient's age, demonstrate that a healthy uterus can often carry a pregnancy even at advanced maternal ages, provided a viable embryo from a young egg is used.¹ Similarly, transferring a chromosomally normal (euploid) embryo, identified through PGT-A, yields high live birth rates that are less dependent on the age of the woman at the time of transfer.⁴³ Both scenarios point to the chromosomal status of the egg/embryo as the critical bottleneck, especially with increasing maternal age. This understanding provides the rationale for fertility preservation (oocyte cryopreservation) at a younger age for those anticipating delayed childbearing.
While cumulative live birth rates demonstrate that persistence through multiple IVF cycles can lead to success for many³⁵, there is a point of diminishing returns. The per-cycle success rate often decreases with each subsequent attempt, particularly for women of advanced maternal age or those with intrinsically poor oocyte quality.³⁶ For women over 40 using their own eggs, the CLBR tends to plateau sooner and at a significantly lower level compared to younger women.³⁶ This necessitates careful and individualized counseling regarding the realistic chances of success with further IVF cycles versus considering alternatives, balancing hope with the financial and emotional toll of repeated treatments.
VII. Visualizing Success: Pregnancy Rates by Age Across Different Approaches
To illustrate the impact of age and treatment type on the chances of pregnancy, the following graph presents approximate success rates. It is crucial to note that these rates are based on different metrics (e.g., monthly natural conception, clinical pregnancy per OS-TI cycle, live birth per IUI cycle, live birth per IVF retrieval) and are drawn from various studies and population data. Direct comparisons should be made with caution, but the overall trends are informative.
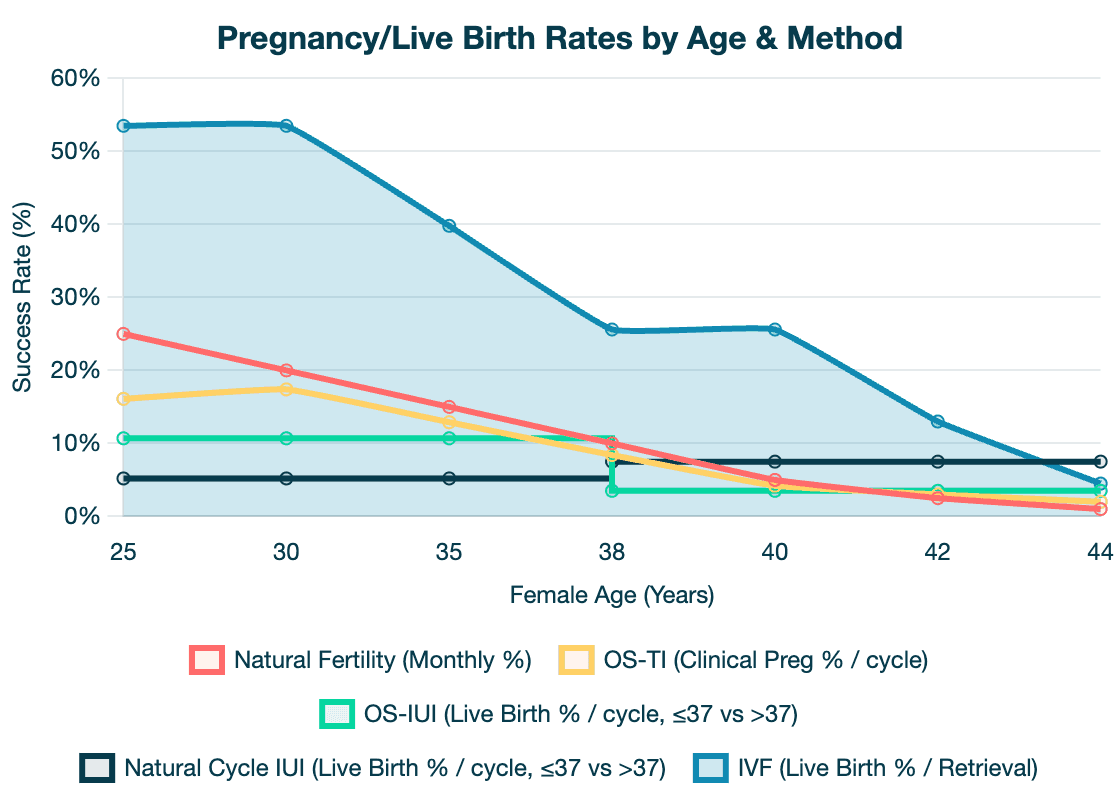
(Graph Description: A line graph would be presented here with "Female Age" on the X-axis (e.g., from 25 to 45 years) and "Pregnancy Rate (%)" on the Y-axis. Separate lines/curves would represent:)
Natural Fertility (Monthly Chance): Starting around 25% at age 25, declining to ~20% at 30, ~12-15% at 35, and <5% at 40. (Data from 1)
Ovarian Stimulation + Timed Intercourse (Clinical Pregnancy Rate per cycle): Starting around 16-17% for ages <35, dropping to ~8% for ages 35-39, and ~4% for age 40+. (Data from 17)
Natural Cycle IUI (Live Birth Rate per cycle): A point/short segment at 5.2% for age ≤37, and another at 7.5% for age >37. (Data from 18)
Ovarian Stimulation + IUI (Live Birth Rate per cycle): A point/short segment at 10.7% for age ≤37, and another at 3.5% for age >37. (Data from 18)
IVF (Live Birth Rate per Intended Egg Retrieval - All Transfers): Starting at 53.5% for age <35, declining to 39.8% for 35-37, 25.6% for 38-40, 13.0% for 41-42, and 4.5% for >42. (Data from 3)
Discussion of Trends and Comparisons:
The visual representation starkly illustrates several key points. Firstly, there is a clear and significant age-related decline in success rates across all modalities that utilize the woman's own eggs. Natural monthly fertility shows a steady decrease, becoming quite low by the late 30s and early 40s.
Ovarian stimulation with timed intercourse (OS-TI) offers a modest improvement over natural monthly chances for younger women with specific conditions like anovulation or unexplained subfertility, but its effectiveness also wanes considerably with age, with clinical pregnancy rates per cycle dropping to single digits for women in their late 30s and beyond.¹⁷
Intrauterine insemination (IUI) success rates also demonstrate this age dependency. The data from Kalu et al. for unexplained infertility shows that ovarian stimulation boosts live birth rates for IUI in women aged 37 and younger (10.7% for OS-IUI vs. 5.2% for Natural Cycle IUI).¹⁸ However, an intriguing finding from the same study suggests that for women older than 37, natural cycle IUI might yield slightly better live birth rates (7.5%) compared to stimulated IUI (3.5%), particularly when clomiphene is used for stimulation (2.1% LBR).¹⁸ This highlights the complexity of ovarian response and endometrial receptivity in older women.
In Vitro Fertilization (IVF) consistently demonstrates the highest per-attempt success rates among the treatments discussed, especially when considering live birth per egg retrieval (which includes all subsequent frozen embryo transfers from that one stimulation).³ Even so, IVF success is profoundly impacted by female age, with rates declining sharply from over 50% for women under 35 to less than 5% for women over 42 using their own eggs.³
The visual disparity in success rates across age groups for all own-egg methods serves as a powerful indicator of the critical influence of time on fertility. This underscores the importance of early consultation and consideration of family planning options, particularly for individuals approaching or in their mid-30s and beyond. The graph can help set realistic expectations for older individuals considering treatment with their own eggs.
Furthermore, the graph illustrates the rationale behind treatment escalation. While less invasive and less costly options like OS-TI and IUI offer a reasonable chance of success for younger women with certain infertility diagnoses, their efficacy diminishes significantly with age. For older women, or those who have not succeeded with simpler treatments, the substantially higher per-cycle success rates of IVF (even with its age-related decline) may present a more efficient, albeit more intensive, path to achieving a live birth. The widening gap in success rates between simpler treatments and IVF as age increases often informs clinical recommendations to consider IVF sooner rather than later, to maximize the window of opportunity while egg quality may still be relatively better.
VIII. Maximizing Your Chances: Key Considerations
Several overarching themes emerge when considering how to maximize the chances of pregnancy, whether naturally or with assistance:
The Overarching Impact of Female Age and Ovarian Health: This cannot be overstated. Female age is the primary non-modifiable factor influencing fertility with own eggs, due to its direct correlation with declining oocyte quantity and, more importantly, quality (increased aneuploidy).¹ Early awareness and planning are key.
The Importance of Male Partner's Fertility: A comprehensive evaluation of the male partner is crucial, as male factors contribute to infertility in a significant proportion of cases. Paternal age, sperm count, motility, morphology, and DNA integrity all play roles that can affect both natural conception and treatment outcomes.⁵
Addressing Specific Infertility Diagnoses: The choice and success of treatment are heavily influenced by the underlying cause of infertility. Conditions like Polycystic Ovary Syndrome (PCOS) or endometriosis present unique challenges and may require tailored treatment approaches to optimize outcomes and manage potential complications.¹² For example, endometriosis can create an inflammatory pelvic environment detrimental to gametes, embryos, and implantation.¹²
The Role of Lifestyle and Preconception Health: Modifiable lifestyle factors—including diet, weight (BMI), exercise, avoidance of smoking, excessive alcohol, and illicit drugs, as well as stress management—can collectively impact fertility in both partners.⁵ Optimizing these factors before and during attempts to conceive can improve natural fertility and may enhance the outcomes of fertility treatments. The cumulative effect of multiple suboptimal lifestyle factors can be substantial.⁶
Understanding Cumulative Success and Multiple Treatment Cycles: For many, achieving pregnancy, especially with treatments like IUI and IVF, is not a single-event success but rather a process that may involve multiple attempts. Cumulative success rates increase with repeated cycles, particularly for younger patients.¹¹ However, it is also important to recognize the law of diminishing returns, especially at advanced maternal ages, where the likelihood of success with further own-egg cycles may become very low.³⁶
IX. Conclusion: Making Informed Decisions on Your Fertility Journey
The journey to achieving pregnancy is unique for every individual and couple, influenced by a complex interplay of biological, lifestyle, and personal factors. This guide has aimed to provide a thorough, evidence-based overview of the chances of conception, both naturally and through various fertility treatments, with a strong emphasis on the pivotal role of female age.
Key takeaways underscore that fertility, particularly when relying on a woman's own eggs, is profoundly age-dependent. Natural conception rates decline steadily from the early thirties, and the success rates of treatments such as Ovarian Stimulation with Timed Intercourse, Intrauterine Insemination, and In Vitro Fertilization also diminish significantly with advancing maternal age. Understanding these statistical realities is crucial for informed family planning and decision-making regarding fertility care.
While population-based statistics offer valuable insights into average probabilities, they do not dictate individual outcomes. Personalized medical advice from fertility specialists is paramount. A comprehensive fertility evaluation can help identify specific factors affecting an individual's or couple's chances and guide the most appropriate course of action. Setting realistic expectations, based on personal circumstances and expert guidance, is essential for navigating the often emotionally and financially demanding path of fertility treatment.
The emotional landscape of fertility challenges can be significant, often involving stress, anxiety, and a sense of uncertainty. Seeking psychological support, connecting with others who have similar experiences, and open communication with partners and healthcare providers are vital components of well-being during this journey.
Reproductive medicine is a dynamic and evolving field. Ongoing research continues to refine existing techniques and explore new avenues to improve success rates and patient experiences. Staying informed about credible advancements, in consultation with healthcare providers, can empower individuals to make the best choices for their unique situation. Ultimately, navigating the path to pregnancy is about combining knowledge with personalized care, realistic hope, and resilient well-being.
Data Reporting Organizations:
Information on fertility treatment success rates is systematically collected and reported by several key organizations:
In the United States, the Centers for Disease Control and Prevention (CDC) manages the National ART Surveillance System (NASS), collecting data from the vast majority of fertility clinics and publishing national summary reports as well as clinic-specific success rates. The latest full data is typically for cycles performed two years prior (e.g., 2022 data released in early 2024/2025).⁷
The Society for Assisted Reproductive Technology (SART), an affiliate organization of the American Society for Reproductive Medicine (ASRM), also reports detailed national summary data from its member clinics in the US, often closely aligning with CDC data.³
In the United Kingdom, the Human Fertilisation and Embryology Authority (HFEA) serves as the independent regulator and collects data on all licensed fertility treatments, publishing annual reports on trends and success rates.³³
In Europe, the European Society of Human Reproduction and Embryology (ESHRE), through its European IVF-Monitoring (EIM) Consortium, gathers and reports ART data from numerous European countries, providing a broader international perspective on treatment utilization and outcomes.²²
Works cited
Facts & Figures | Fertility Statistics - Extend Fertility, accessed May 23, 2025, https://extendfertility.com/your-fertility/fertility-statistics-by-age/
Odds of Getting Pregnant at Any Age Chart, From Age 20-45, accessed May 23, 2025, https://rmanetwork.com/blog/what-are-my-odds-of-getting-pregnant-at-any-age/
National Summary Report - SART, accessed May 23, 2025, https://www.sartcorsonline.com/rptcsr_publicmultyear.aspx
National Vital Statistics Reports - CDC, accessed May 23, 2025, https://www.cdc.gov/nchs/data/nvsr/nvsr74/nvsr74-3.pdf
Lifestyle factors and reproductive health: taking control of your ..., accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3717046/
Effects of lifestyle factors on fertility: practical recommendations for modification - PMC, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC8812443/
ART Success Rates | ART | CDC, accessed May 23, 2025, https://www.cdc.gov/art/success-rates/index.html
Delivery rates in IVF are affected by the age of the male partner - ESHRE, accessed May 23, 2025, https://www.eshre.eu/Annual-Meeting/Geneva-2017/ESHRE-2017-Press-releases/Dodge
Fertility Predictors in Intrauterine Insemination (IUI) - PMC, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10058138/
Intrauterine insemination: prognostic factors - PMC - PubMed Central, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11152422/
Intrauterine Insemination: Fundamentals Revisited - PMC - PubMed Central, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC5676579/
Endometriosis and Infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility - PMC - PubMed Central, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3538128/
IUI Success Rates – Pregnancy by Age - Pinnacle Fertility, accessed May 23, 2025, https://www.pinnaclefertility.com/blog/iui-success-rates-pregnancy-by-age/
Timed Intercourse Guidance - Perch Fertility, accessed May 23, 2025, https://perchfertility.com/fertility-treatments/timed-intercourse/
Timed intercourse, step by step | Fertility Centers of Illinois, accessed May 23, 2025, https://www.fcionline.com/article/timed-intercourse-steps/
Ovarian Stimulation for IVF/ICSI - ESHRE, accessed May 23, 2025, https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Ovarian-Stimulation-in-IVF-ICSI
Timed intercourse in association with controlled ovarian hyperstimulation as the first-line treatment of couples with unexplained subfertility - PMC, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9635603/
Intrauterine insemination in natural cycle may give better results in ..., accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3454991/
Intrauterine insemination in natural cycle may give better results in older women - ResearchGate, accessed May 23, 2025, https://www.researchgate.net/publication/6576505_Intrauterine_insemination_in_natural_cycle_may_give_better_results_in_older_women
IUI Procedure & Success Rates - Pacific Fertility Center Los Angeles, accessed May 23, 2025, https://www.pfcla.com/blog/intrauterine-insemination-iui-procedure-success-rates
IUI Success Rates Explained, How to Improve Them, and More - CNY Fertility, accessed May 23, 2025, https://www.cnyfertility.com/iui-success-rates/
ART in Europe, 2019: results generated from European registries by ..., accessed May 23, 2025, https://pubmed.ncbi.nlm.nih.gov/37847771/
ESHRE 2020 Virtual (5-8 July 2020) Questions for the speakers Session 70: Ovarian stimulation strategies in IVF and IUI, accessed May 23, 2025, https://www.eshre.eu/-/media/sitecore-files/Annual-meeting/Virtual2020/QA/Session-70--Answers.pdf
Intrauterine insemination with ovarian stimulation is a successful step prior to assisted reproductive technology for couples with unexplained infertility - PubMed, accessed May 23, 2025, https://pubmed.ncbi.nlm.nih.gov/34151684/
Relationship between sperm parameters and clinical outcomes of Intra Uterine Insemination (IUI) - PMC, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC7919170/
Success in Pregnancy Through Intrauterine Insemination at First Cycle in 300 Infertile Couples: An Analysis - PubMed Central, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3984651/
Impact of reproductive history on in vitro fertilization and intracytoplasmic sperm injection outcome: evidence from the German IVF Registry - PubMed, accessed May 23, 2025, https://pubmed.ncbi.nlm.nih.gov/12969690/
Impact of recurrent pregnancy loss history on reproductive outcomes in women undergoing fertility treatment - PubMed, accessed May 23, 2025, https://pubmed.ncbi.nlm.nih.gov/35970200/
Assisted Reproductive Technologies patient education booklet ..., accessed May 23, 2025, https://www.reproductivefacts.org/news-and-publications/fact-sheets-and-infographics/assisted-reproductive-technologies-booklet/
ART: Step-by-Step Guide - Society for Assisted Reproductive Technology, accessed May 23, 2025, https://www.sart.org/patients/a-patients-guide-to-assisted-reproductive-technology/general-information/art-step-by-step-guide/
IVF Step-by-step | UR Medicine, accessed May 23, 2025, https://www.urmc.rochester.edu/strong-fertility-center/services/infertility/infertility-treatment-options/ivf/ivf-step-by-step
Deciding how many embryos to transfer: ongoing challenges and dilemmas - PMC, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC5846681/
Fertility treatment 2022: preliminary trends and figures | HFEA, accessed May 23, 2025, https://www.hfea.gov.uk/about-us/publications/research-and-data/fertility-treatment-2022-preliminary-trends-and-figures/
HFEA Fertility Trends & Figures Report - Association of Reproductive and Clinical Scientists, accessed May 23, 2025, https://www.arcscientists.org/reproductive-scientist/hfea-fertility-trends-figures-report/
Cumulative live birth rates after one or more complete cycles of IVF ..., accessed May 23, 2025, https://pubmed.ncbi.nlm.nih.gov/26783243/
Cumulative Live-Birth Rates by Maternal Age after One or Multiple In Vitro Fertilization Cycles: An Institutional Experience - ResearchGate, accessed May 23, 2025, https://www.researchgate.net/publication/337307295_Cumulative_Live-Birth_Rates_by_Maternal_Age_after_One_or_Multiple_In_Vitro_Fertilization_Cycles_An_Institutional_Experience
Donor Egg IVF Success Rates - What Clinics Don't Tell You, accessed May 23, 2025, https://www.eggdonationfriends.com/success-rates-ivf-with-donor-eggs-truth-clinics-dont-tell/
Impact of Various Parameters as Predictors of The Success Rate of In Vitro Fertilization, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9108295/
Factors Associated with In Vitro Fertilization Live Birth Outcome: A Comparison of Different Classification Methods, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC8052806/
Best practices of ASRM and ESHRE: a journey through reproductive medicine - Oxford Academic, accessed May 23, 2025, https://academic.oup.com/humrep/article/27/12/3365/653252
Timed Intercourse Cycle Codes | American Society for Reproductive Medicine | ASRM, accessed May 23, 2025, https://www.asrm.org/practice-guidance/coding-resources/coding/coding-art-clinical-care/timed-intercourse-cycle-codes/
Ovulation Induction Monitoring for IUI | American Society for Reproductive Medicine | ASRM, accessed May 23, 2025, https://www.asrm.org/practice-guidance/coding-resources/coding/coding-art-clinical-care/ovulation-induction-monitoring-for-iui/
Fertility Success Rates - IVF, IUI, & More - CCRM Fertility, accessed May 23, 2025, https://www.ccrmivf.com/fertility-success-rates/
Genetics and Epigenetics of Infertility and Treatments on Outcomes - PMC, accessed May 23, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC6463256/
Diagnosis of Infertility for IVF Procedure | American Society for Reproductive Medicine, accessed May 23, 2025, https://www.asrm.org/practice-guidance/coding-resources/coding/coding-art-clinical-care/diagnosis-of-infertility-for-ivf-procedure/
ART Surveillance - CDC, accessed May 23, 2025, https://www.cdc.gov/art/php/surveillance/index.html
The HFEA Fertility Report 2025: Insights From The Amilis Team, accessed May 23, 2025, https://www.amilis.co.uk/blog/the-hfea-fertility-report-insights-from-amilis
About - ESHRE, accessed May 23, 2025, https://www.eshre.eu/Data-collection-and-research/EuMAR/About
EuMAR - ESHRE, accessed May 23, 2025, https://www.eshre.eu/-/media/sitecore-files/EuMAR/D_FINAL_hoad011.pdf
(PDF) ESHRE PAGES The European IVF-Monitoring Consortium (EIM) ‡ for the European Society of Human Reproduction and Embryology (ESHRE) - ResearchGate, accessed May 23, 2025, https://www.researchgate.net/publication/343760938_ESHRE_PAGES_The_European_IVF-Monitoring_Consortium_EIM_for_the_European_Society_of_Human_Reproduction_and_Embryology_ESHRE
. . .
CARE Fertility and Women’s Health is a leading fertility clinic, offering personalized care and advanced reproductive technology to help individuals and couples achieve their dream of parenthood. With state-of-the-art genetic testing, individualized treatment plans, and holistic support, we specialize in complex fertility cases and boast some of the highest success rates in Canada.
Stay Informed!
Follow us on social media for fertility tips, patient stories, and the latest advancements in fertility care. Facebook | Instagram | LinkedIn | X | TikTok | YouTube